Anesthesia or local anesthesia in dentistry allows you to treat teeth without pain, which provides comfort for the patient and ease of work for the dentist.
Local anesthesia only acts on a limited area and is usually administered by the dentist himself.
Currently, dental treatment without anesthesia is nonsense. Modern medical standards require not only high-quality, but also the most comfortable and painless treatment for the patient. The dentist individually decides how and with what drugs to treat pain, taking into account the amount of work, area, depth and individual characteristics of the patient.
Many of us often delay visiting the dentist because... They have been afraid of them since childhood, but “advanced” caries can cause serious complications that may even require surgical intervention. The smaller the destruction and the earlier the patient consulted a doctor, the better, faster and less painful the treatment can be.
Dentists strongly recommend not to delay your visit. Tooth decay is more dangerous than you think. Possible consequences:
- pulpitis and periodontitis;
- diseases of the cardiovascular system and joints, because caries is a source of infection;
- chronic allergic reactions;
- if the tooth is completely destroyed, this will affect the quality of chewing food and, as a result, may lead to gastrointestinal diseases
Fast Facts About General Anesthesia
Here are some key points about general anesthesia. More detailed and supporting information can be found in the main article.
- The anesthesiologist usually administers a general anesthetic before surgery
- There are some risks associated with the use of general anesthetics, but they are relatively safe when used correctly
- Very rarely, a patient may experience unintentional awakening during surgery
- Side effects of general anesthesia may include dizziness and nausea
- The mechanisms by which anesthesia works are still only partially understood.
General anesthetics cause reversible loss of consciousness and analgesia necessary for surgery . The mechanism of action of anesthetics is not fully understood. There are several theories about this.
General anesthesia is essentially a medically induced coma, not sleep. Anesthetic drugs make the patient indifferent and turn off consciousness .
They are usually administered intravenously or by inhalation . Under anesthesia, the patient does not feel pain and may also experience amnesia.
The drugs will be administered by an anesthesiologist, who will also monitor the patient's vital signs during the procedure.
In this article, we'll look at a number of topics, including the possible side effects of general anesthesia, the risks involved, and some theories about how they work.
What is
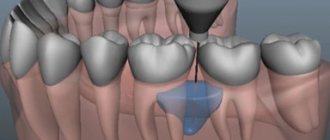
Local mandibular (from Latin mandibula
– lower jaw) anesthesia refers to the conduction method and involves depriving the entire lower jaw of sensitivity. The anesthesia zone covers not only the teeth, but also bone tissue, gums, mucous membranes, the lower lip and even part of the tongue.
Anesthesia according to Bershe-Dubov involves a special method of performing a mandibular blockade. Namely, the place of needle insertion and its advancement. The methodology was developed not as a result of joint work, but separately. But the French doctor Jean Henri Bercher was the first to come up with a special technique in 1922. Soviet dentist M.D. Dubov, based on the practice of his foreign colleague, proposed a slightly different method, which is still used today.
By the way! This blockade is carried out not only during dental operations, but also during painful therapeutic manipulations, for example, when realigning the lower jaw after a fracture or when cutting out an abscess in the anesthesia zone.
Story
General anesthetics have been widely used in surgery since 1842, when Crawford Long prescribed diethyl ether to a patient and performed the first painless operation.
On October 16, 1846, American dentist and surgeon Thomas Morton first administered ether anesthesia to a patient to remove a submandibular tumor.
In Russia, the first operation under anesthesia was performed on February 7, 1847 by Pirogov’s friend at the professorial institute, Fyodor Inozemtsev.
Pirogov himself performed the operation using anesthesia a week later. Over the course of a year, 690 operations were performed under anesthesia in 13 cities of Russia, 300 of which were performed by Pirogov!
Soon he took part in military operations in the Caucasus. Here, for the first time in the history of medicine, he began to operate on the wounded with ether anesthesia. In total, the great surgeon performed about 10,000 operations under ether anesthesia.
Anesthetic solutions
Various compounds are used to innervate the lower jaw. These include lidocaine and novocaine. These substances are time-tested, but are highly toxic. Along with them, articaine anesthetics are used, which give excellent results with less toxicity. These include ultracaine, articaine, ubistezin.
Novocaine is not used in dentistry, since there are more powerful and safer anesthetics of the articaine series. They are 4-5 times superior to novocaine in terms of the degree of analgesic effect.
Articaine drugs, in addition to anesthetic substances, contain vasoconstrictor components such as epinephrine or adrenaline. This ensures that the anesthetic substance remains in the tissues for a long time, since it is not carried by blood vessels outside the area of medical intervention.
Mepivacaine
This short-acting anesthetic is more attractive for patients who have simply had a tooth removed or a cavity filled. After instillation of a long-acting substance, the patient leaves the dentist with numbness in half of his face, and this causes great inconvenience. Loss of sensitivity for 5-6 hours is very unpleasant.
Preparations based on mepivacaine act on tissue for no more than 40-45 minutes, which is quite enough for short dental procedures. The numbness goes away quickly, and the patient can safely eat and drink drinks at the prescribed time without experiencing discomfort.
Medicines based on mepivacaine are recommended for patients with:
- cardiovascular pathologies;
- burdened with allergic anamnesis;
- small carious lesions of molars;
- periodontal pathologies.
Also, short-acting painkillers are indicated for removing surgical sutures, applying bandages, removing intact teeth and other simple manipulations. If the patient only needs to change the iodoform bandage, there is no reason to anesthetize half of the face for 4-6 hours.
Anesthesia during pregnancy
Pregnant women are prescribed anesthesia with drugs that do not cross the placental barrier. That is, they do not penetrate the placenta. These include articaine drugs - ultracaine and ubistezin. The listed solutions also do not pass into breast milk, so they can be used without fear during breastfeeding.
All dental procedures using anesthesia are recommended to be carried out no earlier than the second trimester; in earlier stages of pregnancy, unpredictable complications are possible.
Mandibular anesthesia in childhood
The child’s body is not yet sufficiently adapted to the environment, so the reaction to anesthetics is different. However, it is not recommended to treat children’s teeth without anesthesia due to the risk of severe psychological discomfort and fear. Therefore, anesthetics are used widely and successfully. The dose of administration of the medicinal solution depends on the age of the child and is calculated according to the established formula.
Complications after the use of anesthesia in children are the same as in adults:
- spasm of the masticatory muscles;
- loss of sensation;
- hematoma (bruise);
- swelling of the mucous membrane (allergies).
For children with a mobile nervous system and too excitable, a different type of anesthesia is used - sedation. The child is put into a state of superficial sleep.
Hypnosis as a method of anesthesia
A separate group is represented by verbal manipulation, which includes the method of suggestion - hypnosis. The doctor puts the patient into an altered state by instilling a certain idea. After this, the patient stops experiencing pain. This method is convenient for patients with intolerance to a large number of drugs, as well as with serious damage to the liver and internal organs.
Side effects
Nausea is a common side effect of general anesthesia.
There are a number of potential side effects of anesthesia.
Some people may experience none, others several. None of the side effects are particularly long-lasting and usually occur immediately after anesthesia.
Side effects of general anesthesia include:
- temporary confusion and memory loss, although this is more common in older people
- dizziness
- difficulty urinating
- bruising or soreness from the IV
- nausea and vomiting
- trembling and chills
- sore throat due to breathing tube
Risks
In general, general anesthesia is safe. Even very sick patients can be safely anesthetized. The surgical procedure itself involves much greater risk.
Modern general anesthesia is an incredibly safe procedure.
However, older adults and those undergoing lengthy procedures are most at risk for complications . These findings may include postoperative confusion , heart attack, pneumonia, and stroke.
Some specific conditions increase the risk for a patient undergoing general anesthesia, for example:
- obstructive sleep apnea, a condition in which people stop breathing while sleeping
- seizures
- existing heart, kidney or lung disease
- high blood pressure
- alcoholism
- smoking
- previous negative reactions to anesthesia
- medications that may increase bleeding - aspirin, warfarin , for example
- drug allergy
- diabetes
- obesity or overweight
Unintentional intraoperative awakening
This refers to rare cases where patients report remaining conscious during surgery, long after the anesthetic should have taken effect . Some patients are aware of the procedure itself, and some may even feel pain.
Unintentional intraoperative awakening is incredibly rare, affecting approximately 1 in every 19,000 patients under general anesthesia.
Because of the muscle relaxants used at the same time as anesthesia, patients are unable to let their surgeon or anesthesiologist know that they still know what is happening.
Unintentional intraoperative awakening is more likely during emergency surgery.
Patients who experience unintentional intraoperative awakening may suffer from long-term psychological problems. Most often, awareness is short-lived and only sounds, and occurs before or at the very end of the procedure.
According to a recent large-scale study of this phenomenon, patients experienced involuntary twitching , stabbing pain, pain, paralysis and suffocation, among other sensations.
Because unintentional intraoperative awakening is rare, it is unclear exactly why it occurs.
How is it carried out?
Mandibular anesthesia itself is considered quite complex. And if a dentist undertakes to perform a specific technique (in addition to Bershe and Dubov, V.M. Uvarov, I.V. Berdyuk, P.M. Egorov also proposed their techniques), it means that he is well versed in maxillofacial anatomy and is oriented in the location of the nerve processes responsible for sensitivity.
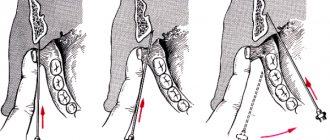
The Bershe-Dubov technique is otherwise called subzygomatic because the injection needle is inserted under the cheekbone. It is noteworthy that this is done externally: the doctor makes a puncture near the patient’s ear.
- First, the lower edge of the zygomatic arch is palpated.
- Then move 2 cm outward from the intertragus notch.
- The injection site is determined under the lower edge of the zygomatic arch.
- A topical anesthetic (for example, lidocaine cream) is applied to this area with a cotton swab.
- A needle is inserted perpendicular to the skin and advanced 2-2.5 cm.
- An anesthetic is released, thereby anesthetizing only the motor branches. This is especially important for trismus (chewing spasms), when the patient cannot open his mouth without pain.
This sequence represents the technique of J. Bercher, who proposed to anesthetize the motor branches of the trigeminal nerve. Dubov supplemented and improved his method.
- To numb the sensitive branches, the needle is advanced another centimeter.
- An anesthetic is administered.
It turns out that if the patient does not have chewing spasms and can open his mouth freely, then there is no need to anesthetize the motor branches. And then the doctor administers anesthesia only according to Dubov. If there is trismus, a general blockade according to Bershe-Dubov is carried out. Pain relief occurs after 15 minutes.
By the way! The dentist must take into account that in order to carry out anesthesia according to Bershe-Dubov, twice as much anesthetic drug should be drawn into the syringe in advance.
Anesthetics for Bershe-Dubov blockade are the most common: those that are widely used in dentistry. This may be lidocaine, articaine, bupivacaine, prilocaine, mepivacaine. The doctor chooses the drug depending on the patient’s medical and allergic history.
Types
There are three main types of anesthesia . General anesthesia is just one of them.
Local anesthesia is another option. It is done before minor surgeries such as toenail removal. This reduces pain in small, focused areas of the body, but the person receiving treatment remains conscious.
Regional anesthesia is another type. It numbs the entire part of the body - the lower half, for example, during childbirth. There are two main forms of regional anesthesia: spinal anesthesia and epidural anesthesia.
Spinal anesthesia is used for operations on the lower extremities and abdomen. The anesthetic is injected through a special very thin needle into the intervertebral space of the lumbar region . Epidural anesthesia is used for long-term pain relief. Can be used for operations on the chest, abdomen, and lower extremities. During an epidural, a thin plastic catheter is inserted through which a local anesthetic is injected. Pain relief can last as long as needed.
Possible complications
The risk of complications when performing anesthesia according to Bershe-Dubov is high, if only because it is a complex technique that requires ideal knowledge of anatomy, as well as practice. In fact, the doctor may miss and insert the needle in the wrong place.
- If it gets into the pterygoid mandibular fold, numbness of the pharyngeal tissue is possible. The patient will immediately feel this and inform the doctor. Immediate administration of a pyrogenal solution will be required, followed by long-term recovery.
- If a vessel is damaged during injection, a hematoma forms. If the doctor does not notice this and administers an anesthetic, then ischemia (decreased blood circulation) of the lower lip and chin also develops.
- When the lingual nerve is damaged, neuritis occurs, which also requires long-term treatment.
If the technique is not followed, the needle may break. If this happens, the doctor should not panic so as not to frighten the patient, otherwise he will begin to twitch and open his mouth, aggravating the situation. You should carefully remove the needle fragment with tweezers, carry out antiseptic treatment of the puncture site and reschedule the operation for another day.
If the needle does get stuck in the insertion area, it can move further due to jaw movement and hit the facial nerves. This can lead to partial facial paralysis. In this case, removal of the needle is possible only after an x-ray.
Local vs General
There are a number of reasons why general anesthesia may be chosen over local anesthesia.
This choice depends on age, health and personal preference.
The main reasons for choosing general anesthesia are:
- The procedure will likely take a long time.
- There is a possibility of significant blood loss.
- This may affect breathing, for example during breast surgery.
- The procedure will make the patient feel uncomfortable.
- It is difficult for the patient to maintain a forced position during surgery.
The purpose of general anesthesia is to induce:
- pain relief or elimination of the natural response to pain
- amnesia or memory loss
- immobility or elimination of motor reflexes
- dream
- relaxation of skeletal muscles
However, the use of general anesthesia poses a higher risk of complications than local anesthesia. If the surgery is minor, then the patient is offered local anesthesia, especially if he has a condition such as sleep apnea or other risk factors.
How long does it last
This depends on the choice of anesthetic. If this is a drug with adrenaline (for example, ultracaine), then the duration of pain relief will be longer (up to 1 hour). Non-adrenaline anesthetics (lidocaine, articaine) have a shorter duration of action (up to 20-30 minutes). In this case, larger amounts of the drug should not be administered in order to increase the duration of pain relief. Otherwise there will be an overdose. In extreme cases, when the operation is not yet completed, and sensitivity begins to return to the patient, repeated anesthesia is performed according to Bershe-Dubov.
If the doctor is experienced and confident in his actions, and the patient completely trusts him and follows all the recommendations (does not move his head or jaw during Bershe-Dubov anesthesia), then everything goes well.
Preoperative assessment
Before undergoing general anesthesia, patients should undergo a preoperative assessment to determine the most appropriate medications, their amount and combination.
Some of the factors that should be examined in the preoperative assessment include:
- body mass index (BMI)
- disease history
- age
- medications taken
- time before anesthesia
- alcohol or drug use
- use of pharmaceuticals
- examination of the oral cavity, teeth and respiratory tract
- cervical spine mobility study
It is important that you answer these questions accurately. For example, if a history of alcohol or drug use is not mentioned, insufficient anesthesia may be given, which could lead to dangerously high blood pressure or unintentional intraoperative awakening.
Stages
The Gödel classification, developed by Arthur Ernest Gödel in 1937, describes four stages of anesthesia. Modern anesthetics and updated methods of drug have improved the speed of onset of anesthesia , overall safety and recovery, but the four stages remain essentially the same:
General anesthesia is similar to a comatose state and different from sleep.
Stage 1 or induction . This phase occurs between the administration of the drug and loss of consciousness. The patient moves from analgesia without amnesia to analgesia with amnesia.
Stage 2, or arousal stage . The period after loss of consciousness, characterized by agitated and delirious activity. Breathing and heart rate become erratic, and nausea, dilated pupils, and holding your breath may occur.
Due to irregular breathing and the risk of vomiting, there is a danger of suffocation. Modern fast-acting drugs are aimed at limiting the time spent on the 2nd stage of anesthesia.
Stage 3 or surgical anesthesia : muscles relax, vomiting stops, breathing is suppressed. Eye movements slow and then stop. The patient is ready for surgery
Stage 4, or overdose : if too much anesthetic has been administered, then depression of the brain stem occurs . This leads to respiratory and cardiovascular collapse.
The anesthesiologist's priority is to get the patient to stage 3 anesthesia as quickly as possible and keep him there throughout the operation.