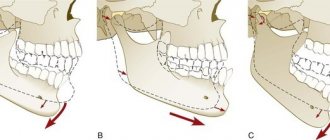
Manifestations of distal bite in the mouth
Closing of lateral teeth during distal occlusion.
Distal occlusion is manifested in the mouth by the closure of the upper and lower teeth according to the “second class” (violation of the relationship between the projections of the antagonist teeth of the upper and lower jaw).
In the frontal segment (at the level of the front teeth) there are two closure options (the so-called first or second subclasses).
In the first case, a “sagittal gap” is observed, which reflects the discrepancy between the dentition in the sagittal plane (anterior-posterior direction). And the upper incisors are in protrusion (inclined forward). In the second option, the upper front teeth are tilted back (into retrusion). With the formation of a deep bite (when the lower teeth are not visible from under the upper ones).
Sagittal chain with distal occlusion. 2 class 1 subclass.
Distal occlusion. 2nd class 2nd subclass.
Which implants to choose?
Today there are more than 3,000 implant systems in the world. However, not all of them can boast a long history of observations and clinical trials around the world. There are also some implant systems that, despite their reliability, are not very common in Russia. This may lead to difficulties in terms of delivery of original components of implant systems.
It is worth choosing only generally recognized implant systems, which are used by different doctors independent of each other. Otherwise, the patient risks finding himself in a situation where no one can help him.
An important point when choosing an implant system is the type of implant-abutment connection. It determines how long the implant will last. The most reliable today is the conical implant-abutment connection with the effect of switching platforms. It is able to withstand greater loads compared to a flat connection, is leak-tight and does not cause resorption of bone tissue around the implant.
The healing of implants is affected by the purity of the titanium from which they are made. The most common is Grade 4 - commercially pure titanium. Grade 1,2,3 alloys are even purer. Grade 5 – less pure, contains impurities of vanadium and aluminum.
The surface of each implant is a unique patented technology, because... It is on the surface of the implant that osseointegration occurs—the fusion of the implant with the bone tissue. Serious implant manufacturing companies conduct a lot of research, proving that their implants are integrated not only in standard situations, but also, for example, in people suffering from diabetes or bleeding disorders. The following systems meet all these requirements: Straumann (Switzerland), Ankylos (Germany), Astra tech (Sweden), Nobel biocare (USA/Sweden). Among the inexpensive systems, we can highlight Osstem implants (South Korea). They have proven themselves throughout the world as a reliable and economical implant system.
Causes of distal bite (distal occlusion)
They are almost always (in the vast majority of cases) skeletal...
- Posterior position of the lower jaw. This is the most common cause of distal occlusion
- Small (short) lower jaw.
Many people write that the cause of a distal bite may be an overdeveloped (excessively large) upper jaw. They say that this is why there is a “gap” between the front upper and lower teeth (sagittal gap)... Many years of observations and our experience have shown that this is not so. With any anomaly of occlusion, there can be no talk of any OVERdevelopment. Everything, on the contrary, is UNDERdeveloped.
The lower jaw ends up in a posterior position (the first reason) only because the lower teeth bump into the upper teeth while the upper jaw is shortened and narrowed (generally underdeveloped). Or, when the upper incisors are “wrapped” back, into retrusion (second subclass). In addition, with distal occlusion, the upper jaw is always narrower than the lower jaw. Which, by the way, is another reason for blocking the lower jaw in the posterior position. And this same “blocking” does not allow the lower jaw, which is caught in the trap, to develop normally. Here is the second reason for distal occlusion - underdevelopment of the lower jaw.
There is also a “dental” reason for distal occlusion. Or more precisely, the dental cause of closure is “second class”. This is when mesial (front) displacement of the upper lateral teeth occurs. And then, even with a normal relationship of the jaws in the sagittal plane, the closure of the lateral teeth (molars) will also be in the second class. True, this is not a true distal occlusion...
A “dental” cause of the second class may complement or may camouflage true distal occlusion. Therefore, it will not be possible to figure out what is the reason for the closure in class 2 visually (by eye). Diagnostics required.
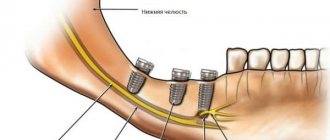
Why and how osteoplasty is performed
Bone grafting is necessary when the available volume of bone tissue is not enough to create reliable support for a dental implant. It is carried out in the following ways:
- Sinus lift. Indicated only for the upper jaw in the area of the chewing teeth, above which are the maxillary sinuses. Access to the bottom of the sinus is created in the bone, the sinus membrane is lifted with special instruments, and the resulting space is filled with osteomaterial. The operation is performed using an open or closed method. The first is more traumatic and is used when it is necessary to significantly increase the size of the bone. Simultaneous installation of implants is possible if the thickness of the remaining bone is at least 4 mm. Otherwise, sinus lifting is carried out in a separate preliminary stage. The recovery period takes 5-6 months.
- Bone grafting (BMG). Relevant for small defects. The graft used is xenogeneic material based on bovine bone or synthetic materials that stimulate growth. To give the desired shape and protection from external factors, the area to be grown is covered with a barrier membrane. The procedure is low-traumatic, but financially expensive.
- Bone block transplantation. It involves transplanting the patient’s own jaw block, taken from other parts, into the problem area. The bone block is fixed with ultra-thin screws and covered with a collagen membrane. It takes 6-8 months to survive. In our Center, the method is not used because it is traumatic and requires additional surgical intervention to collect material.
- Splitting of the alveolar ridge. Allows you to increase the jaw bone only in thickness. A cut is made in the middle of the bone, which is expanded with special tools. Then the implant is fixed into the resulting gap, and the space around is filled with osteomaterial. Rehabilitation after surgery takes up to 4 months. We do not use this technique due to increased trauma and the risk of non-healing of the titanium structure.
Bone grafting with further tooth implantation
Diagnostics
The main goal of any diagnosis is to identify the cause of the problem. And make a diagnosis. Likewise, the diagnosis of distal occlusion is designed to identify the cause of closure in the second class. In order to separate the flies from the cutlets during treatment, so to speak. That is, dental causes of closure are in the second class from non-dental (maxillary, skeletal).
The main diagnostic methods are:
- Analysis of TRG (teleradiogram) of the skull in a lateral projection. It allows you to clearly determine all the skeletal (jaw) nuances of the problem. Both with the position of the jaws and with their sizes.
- Analysis of plaster models of jaws (for this, casts are taken). It allows you to clarify the “dental” nuances: the size of the teeth, the length and width of the dentition, the features of the relationship (including closure) of the upper and lower teeth
Analysis of TRG (teleradiogram) of the skull in a lateral projection.
Analysis of plaster models of jaws.
It is not recommended to fall below this diagnostic “bar”. Below - just by eye. But this, as we understand, is not the best option.
Diagnostics is the first and key step in the treatment of distal occlusion. Do you want to know why it’s impossible to do without diagnostics?
What can replace implantation?
Implantation is the only method of restoring lost teeth that stops bone resorption. But there are cases when surgery is contraindicated or a person is not financially ready to undergo surgery. As an alternative from an aesthetic and functional point of view, the following are used:
- Removable dentures. They consist of a plastic base that serves as the gum and artificial teeth attached to it. Made from acrylic or nylon. Service life - 5-10 years. Due to improper load distribution, they put increased pressure on the gums, sag, and require constant relining. The jawbone under such prostheses is actively decreasing.
- Bridges. Several crowns welded together, the outermost of which are attached to the previously ground living teeth adjacent to the defect. Made from metal ceramics or zirconium dioxide. The average service life is 7 years (depending on the condition of the supporting units). Due to uneven pressure, the bone in the defect area is resorbed.
We recommend not to delay the restoration of the dentition and consider implantation as an effective way to stop the process of bone tissue atrophy. Complete resorption over time makes any type of prosthetics almost impossible.
Errors in the treatment of distal occlusion
The first, main mistake is that many try to treat distal bite with one device. For example, only with braces (this is the most popular option). But braces, although a cool device, are not for skeletal problems. The level of hardware competence of the braces system does not extend further than “to place the teeth on the jaw.” And distal occlusion, as we have already said, is a purely skeletal problem. Jaws and posture are to blame. And braces are not capable of solving problems with posture or jaw problems. After all, braces cannot change the position or size of the jaw. No matter what the would-be doctors promise...
And therefore, such videos are just an advertising gimmick.
Or rather, a convenient “hook” that catches gullible patients. Convenient because it coincides with the desire to do everything quickly and efficiently... But it doesn’t coincide with reality.
And braces cannot be the main device in the treatment of distal occlusion.
Braces are the wrong choice when treating distal malocclusions. In any case, you definitely shouldn’t start with them. Braces, as mentioned and shown above, can be effectively used only at the final stage of treatment of distal occlusion. All major “feats” must be accomplished before working on the teeth. Before using braces. And they are accomplished at the level of the jaws and skeleton (posture). Otherwise, there will simply be nothing to “clog” (close) these teeth (read with braces). See “Fundamentals of the therapeutic concept of “Ortho-Arteli”.
The second common mistake in correcting distal occlusion is treatment with the removal of upper premolars (4 or 5 teeth).
And this mistake is much more serious. Because it can have the most dire consequences. See "Orthodontic treatment with tooth extraction."
After all, as we said above, the main causes of distal occlusion are skeletal. And most often the lower jaw is to blame. And if so, then a reasonable question arises: if the lower jaw is to blame, what does the upper teeth have to do with it (their removal). Where is the logic?
In general, all errors in the treatment of distal occlusion in an adult are usually associated with insufficient diagnosis. Which entails a misunderstanding of the reasons for the occurrence of distal occlusion in each specific case.
For example, the “dental” cause of distal occlusion is very often confused with the “skeletal” (jaw) cause. We remind you that in the first case you need to move the lateral teeth back. And in the second - to push the lower jaw forward and develop the upper one. And if you get confused, if you don’t figure it out... Start distalizing the upper teeth, or worse, remove them when it is necessary to advance the lower jaw... Or vice versa. It is clear that nothing good will come of it.
The third mistake is when, without understanding what’s what, what exactly is the cause of distal occlusion, but realizing, however, that the problem cannot be corrected with braces, they try to solve the problem surgically. Using orthognathic surgery. Through osteotomy of the lower and upper jaws.
This is where I would like to dwell in more detail. And explain something. Why do orthodontists send to a surgeon to “treat” a distal bite? They have already said: they understand that braces will not cope. But they don’t understand how to treat it without braces. They don’t understand because in dentistry in general, and orthodontics in particular, there are a lot of prejudices regarding the possibilities of moving the lower jaw forward and developing the upper jaw. And these, as we saw above, are the main (“key”) points in the treatment of distal occlusion.
Most orthodontists simply do not believe in this (that it is possible in principle). Because someone (even a “great one”) said two hundred years ago that this cannot be done. Time has passed. Everyone has already forgotten why it is “impossible”. But no one even bothered to check why, in fact, it was impossible...
And therefore, those doctors who blindly believe in these moss-covered “dogmas” simply do not see an alternative. And for them there are only two extreme poles in the treatment of distal occlusion: braces and surgery. That's all.
During a direct examination by a specialist, you will be able to find out your exact diagnosis, as well as receive a referral for diagnosis or a treatment plan.
And in our clinic we treat distal occlusion between these two poles. Using methods of maxillofacial orthopedics and craniodontics. Here are the ones: changing the position of the lower jaw and changing the size of the upper. And we get good results, without regard to the fact that someone once said something... We must always double-check what was said. We checked. And everything turned out to be somewhat different. Or rather, not at all the way they “frightened” us. You can also push it out. It can be developed. You just need to know how, because there are some “secrets” here. And we, at the Orto-Artel clinic, knowing these “secrets”, take advantage of these opportunities, successfully eliminating distal occlusion of any complexity.
By the way, if we are talking about surgical treatment of distal occlusion, then we need to determine when and in what cases surgery is generally appropriate. But the indication is basically the same - a small lower jaw, the so-called lower micrognathia, and the micrognathia is very pronounced.
We indicated this reason above as one of the skeletal reasons. I will add: the lower jaw should be VERY short. Literally ugly. Only then can this be resolved surgically. In all other cases, you can do without surgery. Proven and tested many times.
By the way... In our clinic, a good half of the patients have formal indications for surgical treatment of distal occlusion. But only a few got to the surgeon. Because formalities are formalities, but compromise solutions were found that satisfied everyone: both the patients and us. This is because we approach treatment not formally, but in essence. And we are guided by logic and common sense.
Well, as a special case of a short lower jaw, which cannot be corrected except by surgery, this is a small chin. If it is small and spoils the face, then even by pushing the lower jaw forward we will not get the aesthetics we want. Simply because orthodontists do not have the means and instruments (devices) to selectively influence the chin. It is impossible to stimulate the chin to grow. Only surgery.
Inferior micrognathia.
This is where the indications (and there is essentially one) for surgical intervention for distal occlusion end.
Going with a knife into the upper jaw - God forbid! Even if the upper jaw is indirectly to blame for the distal occlusion. More precisely, the upper jaw also, as a rule, suffers (dimensionally) with distal occlusion. The upper jaw is directly connected to the base of the skull. And such interventions can then backfire. Literally. And the most important thing is that there is no need to go there surgically. The upper jaw can be developed!!!
Why does bone loss occur?
When teeth are lost due to lack of natural load, the jaw bone atrophies. The process is activated 3 months after removal and reaches its climax within a year. Among the secondary reasons for the reduction of bone tissue in size:
- chronic inflammatory diseases of the oral cavity;
- age-related weakening of the tissues surrounding the tooth in older people;
- congenital pathologies of the dentofacial apparatus;
- jaw injuries;
- dentures supported by living teeth or gums.
Bone resorption leads to the following consequences:
- psychological discomfort due to a gap in the dentition, difficulty eating;
- change in the shape of the face: the appearance of wrinkles in the mouth, sagging cheeks, displacement of the chin, sunken lips;
- the need to reline a removable denture when using it.