Trigeminal neuritis is sometimes mistakenly called trigeminal neuritis of the facial nerve, but more often another term is used - “neuralgia” - which literally means pain. This is an inflammatory process in the fifth pair of cranial nerves.
Our expert in this field:
Vasinkina Inna Yurievna
Neurologist
Call the doctor Reviews about the doctor
Some facts about the disease:
- On average, it occurs in 6-8 people out of every 100,000.
- Women get sick more often than men.
- In most cases, the disease is diagnosed in people over 40-50 years of age.
There are two types of trigeminal neuralgia:
- Primary occurs as an independent disease.
- Secondary – a symptom of other pathologies.
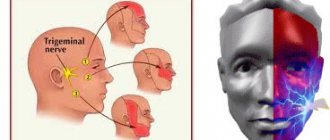
How does the trigeminal nerve work?
The trigeminal nerve is the fifth pair of cranial nerves (there are 12 pairs in total - they innervate the organs of the head and neck). It is paired - that is, it is on the right and left. It consists of two types of nerve fibers - sensory and motor. After exiting the skull, the trigeminal nerve divides into three branches, which seem to cover the entire face:
- Ocular - is sensitive, innervates the eyeballs, eyelids, lacrimal sacs, mucous membrane of the nose and its paranasal sinuses, lacrimal gland, forehead skin.
- Maxillary - also sensitive, innervates the skin of the cheek, temple, teeth and gums of the upper jaw, mucous membrane of the palate, nose.
- Mandibular - responsible for both sensitivity and movement, innervates the muscles of mastication, muscles of the palate, eardrum, mucous membrane of the cheek, anterior 2/3 of the tongue, skin of the temple, the front of the ear and external auditory canal, teeth and gums of the lower jaw.
Signs of trigeminal neuralgia
A typical symptom of trigeminal neuralgia is prosopathy - facial pain. The sensation can be compared to an electric shock. Pain of a paroxysmal nature lasts 5-15 seconds and occurs abruptly. It is usually localized in the area of the lower jaw and cheekbones, but can appear in any part of the face. Neuralgia in severe form leads to partial or even complete loss of sensitivity.
Other symptoms:
- nervous eyelid tic;
- impaired coordination of movements;
- increased body temperature;
- headache;
- chills, fever;
- general weakness.
Treatment of trigeminal neuritis
Typically, treatment of the disease begins with medications:
- Anticonvulsants . Usually the drug carbamazepine or phenytoin, oxcarbazepine is prescribed; the doctor selects the dose individually. Over time, these medications may become less effective, in which case your doctor will increase the dosage. However, anticonvulsants have some side effects that may make it difficult to use them.
- Antispasmodics . Used together with anticonvulsants. For example, a neurologist may prescribe baclofen for you.
- Physiotherapy . Diadynamic currents, ionogalvanization with novocaine, and ultraphonophoresis with hydrocortisone help to cope with the symptoms of trigeminal neuritis.
If neuralgia manifests itself in the form of severe toothaches, painkillers are used, and ointments with anesthetics are rubbed into the gums.
If medications no longer help, the neurologist raises the question of surgical treatment of trigeminal neuritis. The following operations are possible:
- Microsurgical decompression . During the intervention, compression of nerve fibers by blood vessels is eliminated. Typically the incision is made behind the ear. The operation effectively eliminates pain, but after it a relapse may occur, complications such as hearing loss, numbness of the face, paresis and paralysis of the facial muscles.
- Transection of nerve branches . In this case, the transmission of pain impulses is disrupted.
- Radiosurgery (gamma knife). A special device generates a high dose of ionizing radiation, which damages nerve fibers. If painful attacks begin to bother you again in the future, the procedure can be repeated.
There are other surgical methods for treating this type of neuritis.
We will call you back, leave your phone number
Message sent!
expect a call, we will contact you shortly
The trigeminal nerve provides sensation to the skin of almost the entire face and front of the head. It is mixed in structure, that is, it is responsible for both sensitivity and movement, but the motor fibers are thinner. Still, the trigeminal nerve is mostly sensitive. This determines the characteristics of the symptoms of the disease.
Types of neuralgia
Neuralgia that develops as a result of viruses and other diseases is called secondary. Primary or idiopathic is a disease caused by compression of a nerve. According to localization, it can be unilateral or bilateral. With unilateral neuralgia, one branch of the nerve is affected, with bilateral neuralgia, several.
According to the nature of the disease, it can be acute or chronic. With acute neuralgia, the patient experiences frequent and severe pain. If the pathology is not treated, it goes into a chronic stage, when exacerbation is replaced by periods of remission.
Postherpetic neuralgia develops after herpes and differs from the classic nature of the pain, which may not go away for several hours. An atypical form of neuralgia is a psychosomatic disease, which can be triggered by stress, depression, and nervous exhaustion.
Methods for diagnosing neuralgia
The disease is diagnosed using different methods that make it possible to establish its cause:
- visual examination and questioning of the patient;
- radiography;
- MRI of the head;
- biochemical studies of blood and urine;
- electromyography.
To clarify the diagnosis, the neurologist often turns to doctors of other specialties - otolaryngologist, ophthalmologist, orthodontist. This is done to exclude diseases for which the same symptoms are typical.
Drug treatment of neuralgia
Effective treatment is only possible with the use of a comprehensive drug regimen. Anticonvulsants are prescribed first. Antihistamines and local analgesics are sometimes added to them to relieve acute attacks of pain. The deficiency of gamma-aminobutyric acid will be compensated by phenibut and similar neotropic drugs. In case of exacerbation, antidepressants may be prescribed. If the disease is caused by a viral infection, the patient is prescribed non-steroidal antiviral and antibacterial drugs.
Other treatments
To eliminate pain, physiotherapeutic procedures are prescribed: acupuncture, magnetic therapy, ultraphonophoresis. A good addition to drug treatment is head and face massage. If conservative treatment methods do not bring the desired effect, the patient may be prescribed a minimally invasive operation - microsurgical decompression, radiosurgery or percutaneous destruction.
Trigeminal neuralgia is not only painful, but also causes problems with the patient’s communication abilities. Constantly expecting attacks of pain, a person isolates himself from others, withdraws into himself, becomes irritable and depressed. The prognosis for treatment is favorable. The chances of a full recovery increase when the patient consults a doctor at an early stage of the development of neuralgia, when the first symptoms appear.
What are the symptoms of trigeminal neuritis?
I am bothered by excruciating attacks of shooting, stabbing pains. They usually last for a few seconds or minutes and then suddenly go away. Most often, pain occurs in the area of innervation of the two lower branches of the trigeminal nerve: in the jaws, cheeks, teeth, gums, lips. In the area of innervation of the upper first branch of the nerve (forehead, eyes), pain occurs less frequently.
Usually only the right or left half of the face is affected. During an attack, a grimace of pain appears on the face, the person freezes, is afraid to move, and holds his breath. Sometimes the patient, on the contrary, begins to breathe heavily and frequently and rubs the sore spot.
Over time, attacks become more frequent and severe. There are certain “trigger zones” - most often they are on the lips and gums. Touching them, exposure to high or low temperature (cold or hot food) provoke painful attacks.
Often, pain due to neuritis is accompanied by vegetative symptoms, such as redness of the facial skin, lacrimation, and the release of large amounts of saliva.
Are you experiencing similar symptoms? Perhaps this is trigeminal neuritis or another disease, for example, arthrosis of the temporomandibular joint, multiple sclerosis. Only an experienced neurologist will be able to establish the correct diagnosis and prescribe effective treatment.
Tooth pain due to neuralgia, causes and treatment
The presence of toothache does not always indicate problems with the teeth and oral cavity. Sometimes tooth pain can occur in people with completely healthy teeth. In this case, there is a possibility that toothache is a symptom of trigeminal neuralgia, which is hidden behind such pain, making it difficult to identify the real cause of the ailment.
The trigeminal nerve is one of twelve pairs of cranial nerves, which is a continuation of the spinal cord and is responsible for the functioning of many reflexes, such as blinking, sneezing, and eyebrow movements. Also, together with others, this nerve ensures normal breathing. The trigeminal nerve consists of three branches that form it: the first branch is located at eye level, the second above the upper jaw near the nose, and the third in the lower jaw.
There are two types of trigeminal neuralgia - true and secondary. True or primary neuralgia is a self-limiting disease, while secondary neuralgia develops due to the presence of complications of other diseases. The type of inflammation can be determined based on a number of reasons that caused the development of trigeminal neuralgia.
Reasons for the development of true neuralgia:
- displacement of arteries and veins;
- the presence of adhesions or tumors;
- injury to the face.
Causes of secondary neuralgia:
- gingivitis;
- pulpitis;
- periodontitis;
- periostitis;
- after tooth extraction:
- dental caries;
- in the presence of ENT diseases;
- in case of metabolic disorders;
- after hypothermia, etc.
The manifestations of symptoms of trigeminal neuralgia depend on which branch is affected. Toothache, as well as pain in various areas of the head, occurs when the second and third branches become inflamed. However, the nature of the pain differs depending on the inflamed branch, which helps to determine the affected area. With neuralgia of the second branch of the trigeminal nerve, pain manifests itself in the area of the nose, facial muscles and the entire upper row of teeth, while, as with inflammation of the third branch, pain in the neck, chin, cheeks, and lower teeth is characteristic.
The main symptoms of inflammation of the trigeminal nerve:
- paroxysmal toothache, radiating deep into the bones;
- spasm of the facial muscles during an attack;
- discomfort when eating hot or cold food, when brushing your teeth, as well as when touching your face, etc.
If you experience toothache associated with neuralgia, you must consult a doctor. However, if the pain is due to inflammation of the trigeminal nerve, your dentist will most likely not be able to help you. For qualified help, you need to go to a neurologist to avoid the development of complications and not to aggravate the situation.
Long term forecast
With treatment (and in rarer cases, without it), remission - the symptoms of trigeminal neuritis do not bother you for several months or even years. Many patients are helped by medications, but over time they begin to act weaker, and they have to resort to surgical treatments.
Frequent and severe pain attacks can reduce performance and quality of life. In young patients, the prognosis is more favorable, in older people (and it is in them that the disease occurs more often) it is more serious.
We will call you back, leave your phone number
Message sent!
expect a call, we will contact you shortly
The cause of trigeminal neuritis is not always found. In this case, the disease is called idiopathic . If the damage to the nerve trunks is caused by some other disease, they speak of symptomatic , or secondary , neuritis.
Most often, the disease develops as a result of compression of the nerve by improperly located vessels. In most cases, the superior cerebellar artery is to blame.
Modern medicine sees the mechanism for the development of inflammation and pain as follows. Chronic compression causes the trigeminal nerve to lose myelin , a sheath that is made of fat and is important in conducting nerve impulses. An inflammatory process develops. Subsequently, degeneration of axons - the long processes of nerve cells that make up the nerve fiber.
What is a dental nerve?
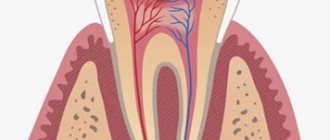
Simply put, the dental nerve is a neurovascular bundle that is located inside the teeth or in the tissues surrounding the tooth. Simply put, this bundle is also called pulp.
The pulp is needed to ensure the vital functions of the tooth; it helps supply the canine with essential vitamins and minerals. Protects dentin from the penetration of bacteria, prevents the formation of pathogenic flora in the unit.
When the nerve is removed, the tooth becomes essentially “dead.” That is, he does not receive the necessary nutrition. Over time, it will lose its strength, may change color, dentin will become thinner, so these manipulations are done only as a last resort.
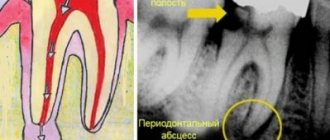
What is tooth nerve inflammation?
This pathology is caused by an advanced stage of caries. If a person does not go to the dental clinic in time, then bacteria will gradually destroy dental tissues, eventually reaching the pulp, which leads to pulpitis.
Pulpitis
is an inflammatory process in the tissues of the dental unit.
Treatment of pulpitis always begins with removing the nerve of the tooth and cleaning the canals.
What other causes can lead to trigeminal neuritis?
In addition to vascular compression, other causes can lead to the disease:
- Age-related changes in the body.
- Compression of the nerve branches in the bone canals of the skull in which they pass. These canals can be narrowed from birth, or as a result of certain diseases: caries, sinusitis.
- Compression by intracranial tumors.
- Injuries to the face, head.
- Multiple sclerosis. This is a chronic disease in which the myelin sheath is destroyed. Trigeminal neuritis affects 3-4% of patients with multiple sclerosis.
- Postherpetic neuralgia. Its cause is herpes zoster.
Causes of neuralgia
Unlike neuritis, which is an inflammatory disease, neuralgia is not. Neuritis develops against the background of a virus and infection. Neuralgia occurs due to mechanical effects on the trigeminal nerve, provoked by various factors.
- Head injuries with displacement of the skull bones.
- Tumors of various etiologies, which, as they grow, compress the trigeminal nerve.
- Bite defects and other anomalies of the dentofacial area.
- Diseases of blood vessels located in close proximity to the trigeminal nerve.
- Chronic sinusitis and otitis.
- Medical error during tooth extraction.
- Neuralgia can be triggered by infections, including periodontitis, stomatitis, herpes, and syphilis.
Hypothermia does not cause neuralgia, but makes treatment difficult. Neurosis, metabolic disorders, diabetes mellitus and other chronic pathologies have a negative effect on therapy.
Causes of pain attacks in trigeminal neuritis. What are triggers?
Triggers are irritants, “triggers” that provoke an attack of pain. These can be a variety of mechanical or temperature effects on the skin of the face and mucous membranes.
Most often, the following factors act as triggers: shaving, eating food (especially cold or hot), any touching the face, drinking, talking, brushing teeth, wind, applying makeup, washing, smiling. When habitual daily actions always lead to excruciating pain, this significantly reduces the quality of life and interferes with work.
When you see your doctor, tell your doctor what triggers lead to attacks in your case.
How does the treatment of neuritis depend on the causes?
If the cause of trigeminal neuritis is not known, all that remains is to deal with its main manifestation – pain. The neurologist prescribes various medications, and if they stop helping, he recommends surgery.
If the cause of the disease is known, you need to try to eliminate it. For example, if a patient is diagnosed with multiple sclerosis, special therapy is prescribed that helps slow down the progression of the pathology. If the nerve is compressed by an artery or the walls of a bone canal, the compression must be removed.
We will call you back, leave your phone number
Message sent!
expect a call, we will contact you shortly
Sometimes, before the correct diagnosis is finally established, a patient suffering from trigeminal neuritis has to see more than one doctor. It is extremely important to start treating the disease as early as possible. It has been proven that the longer a person suffers from trigeminal neuralgia, the more difficult it is to cope with the pathology.
Diagnosis of trigeminal neuritis: what happens during an appointment with a neurologist?
An appointment with a doctor begins with a conversation. First of all, it is important for a neurologist to get answers to three questions:
What is the nature of the pain? Is it typical for this disease ? With trigeminal neuritis, pain attacks occur suddenly, they are strong, painful and pass quickly.
Where does the pain occur ? When the trigeminal nerve is damaged, pain is localized on the face, in certain places.
What triggers lead to seizures ? Usually this is touching the face, exposure to wind, high and low temperatures.
You will be asked how long you have been experiencing symptoms, whether you suffer from any chronic diseases, and whether you are receiving any treatment. Then the neurologist will examine you and press on certain points on your face where the branches of the trigeminal nerve enter the skin. A general neurological examination will be performed to diagnose any possible medical conditions that may be causing your symptoms.
Comparative analysis of the effectiveness of complex pharmacotherapy for pain in trigeminal neuralgia
Pain in the facial area can be caused by damage to the nervous system of the maxillofacial area (the system of the trigeminal, glossopharyngeal nerves, autonomic ganglia and plexuses) or muscle-articular dysfunction due to arthrosis of the temporomandibular joint and a violation of the relationship of the dentition. In addition, rhino- and ophthalmogenic prosopalgia have been described, the pathogenesis of which is complex, but ultimately realized through neurogenic and muscular mechanisms.
In clinical practice, the most common cranial neuralgia is trigeminal neuralgia, or trigeminal neuralgia (TN). The prevalence of NTN is 45–50 per 100 thousand population with a peak incidence in the 6th decade of life. The pathogenesis of the disease is complex. It has been proven that the trigger point is a radicular-vascular conflict in the area of the cerebellopontine angle, leading to segmental demyelination of the trigeminal nerve root. The combination of root demyelination with functional and/or structural defects in antinociceptive regulatory systems in a given individual may contribute to the formation of the so-called “generator of pathological activity” in the trigeminal nerve system and serve as the basis for the development of the clinical picture of NTN [5].
Clinical picture of trigeminal neuralgia
Patients complain of paroxysmal pain comparable to an electric shock. The duration of the painful paroxysm does not exceed 2 minutes, although patients may complain of continuous pain. However, upon careful questioning, it is possible to establish the presence of a “light” pain-free interval between attacks.
Characteristics of painful paroxysm:
1. The pain is extremely severe and, when determining its intensity on a 10-point pain scale, corresponds to 8–10 points.
2. The pattern of pain during an exacerbation does not change (pain cannot move to the opposite side) and corresponds to the radicular-segmental zone of innervation.
3. Between two separate attacks there is always a pain-free (refractory) period.
4. The presence of trigger zones - hypersensitive areas on the skin of the face or in the oral cavity, slight irritation of which causes a typical pain attack. Trigger zones are most often localized in the medial parts of the face or on the alveolar processes of the jaws.
5. The presence of trigger factors - actions or conditions under which typical pain paroxysms occur. The most common factors are: washing, eating, movements of the lower jaw.
6. Typical pain behavior - during an attack, patients “freeze” in the position in which the attack caught them.
7. At the height of the attack, there may be twitching of the facial muscles.
8. Absence of a sensory defect on the face at the onset of the disease.
During a clinical neurological examination, a decrease in vibration sensitivity and corneal reflex may be noted on the pain side. Also, during an exacerbation of NTN in the presence of active trigger zones, the Sternberg symptom is positive - indicating the localization of the trigger zone, the patient does not touch the face for fear of causing an attack.
The course of the disease is chronic. In 2/3 of patients, at the onset there are mild paroxysms of pain in the projection of the teeth, which may be a reason for their removal; in 1/3, already at the beginning of the disease, paroxysms of intense pain develop, which last 2–3 weeks. and go away on their own. As a rule, after six months or a year, attacks recur in a more severe form. In the advanced stage of the disease, exacerbations (periods of intense pain), which develop more often in the cold season, last 4–8 weeks, then subside, but do not completely go away without adequate treatment. At the beginning of the disease, remission (the period of subsidence of pain) can be spontaneous, however, as our clinical experience shows, over time they can be achieved only with adequate therapy.
As the disease develops, probably due to the increase in the demyelinating process in the area of the trigeminal nerve root, the neuropathic stage of neuralgia is formed, when the clinical picture, along with paroxysms of pain, shows slight constant pain. At this stage, clinical neurological examination reveals a permanent or transient peripheral sensory defect in the area of innervation of the second and/or third branches of the trigeminal nerve.
Diagnosis of typical NTN does not present significant difficulties, however, it should be remembered that paroxysmal prosopalgia can be symptomatic, i.e., caused by pathological processes in the area of the cerebellopontine angle (tumor of the vestibulocochlear nerve, adhesive meningeal process, etc.). In this regard, patients with newly diagnosed NTN under the age of 50 years, as well as with the presence of symptoms of focal damage to the nervous system in their neurological status, require an MRI examination of the brain.
Treatment of trigeminal neuralgia
Treatment of pain in NTN is still a difficult task. In 1962, S. Blum proposed treating trigeminal neuralgia with carbamazepine. Currently, along with carbamazepine, other antiepileptic drugs are used: gabapentin, oxcarbazepine, pregabalin (Lyrica).
It is recommended to start treatment with carbamazepine with 50 mg (1/4 of a standard tablet containing 200 mg of carbamazepine) 3 times a day during or after meals, with a sufficient amount of liquid [3]. If well tolerated, the dose of carbamazepine can be increased by 50 mg daily. The average effective dose is 600–800 mg/day. The dose is considered effective if the pain syndrome is completely relieved (irritation of trigger zones and trigger factors do not cause painful paroxysm - the patient can eat and painlessly perform hygienic procedures of washing and brushing teeth).
Further treatment for 3–4 weeks. is carried out using an individual effective dose of the drug, which allows you to achieve drug remission. Then a back titration is carried out with a decrease in the daily dose by 50 mg over 5–7 days. The goal of back titration is to achieve an individualized maintenance dose, which can range from 100 to 400 mg/day. At the onset of the disease, some patients (40–60%) manage to completely discontinue the drug. It is possible to use prolonged pharmacological forms of carbamazepine, which are especially convenient for maintenance therapy.
When treating with carbamazepine drugs, it should be remembered that long-term use of large doses can lead to the development of side effects such as dizziness, nausea, and ataxia. Cases of aplastic anemia have been described. Therefore, along with clinical monitoring of the development of possible side effects of the drug, it is necessary to monitor the condition of peripheral blood and liver (complete blood count and AST and ALT levels every 3 months).
In approximately 15% of patients, carbamazepine is ineffective. For such patients, antiepileptic drugs of other groups are selected.
Currently, the basic principles of rational polypharmacotherapy have been formulated, suggesting an impact on the main pathogenetic mechanisms of neuropathic pain in NTN: peripheral and central sensitization with simultaneous activation of the antinociceptive system [5]. Treatment regimens for neuropathic pain use local anesthetics that block the conduction of pain impulses at the peripheral level, which is technically impossible in case of NTN; opioid analgesics that have a central effect, and adjuvant analgesics, which include antidepressants that enhance the inhibitory effect of antinociceptive systems, and antiepileptic drugs that inhibit the conduction of nociceptive stimuli at the segmental and suprasegmental levels. The effectiveness of drugs used in various combinations in the proposed regimens varies [3]. In this regard, studying the effectiveness and safety of the use of pregabalin (Lyrica) and carbamazepine in the complex treatment of NTN seems timely and relevant.
The purpose of this study is to improve methods of complex treatment of patients suffering from NTN in the acute stage, through a comparative analysis of the therapeutic effectiveness of pregabalin (Lyrica) and carbamazepine in complex treatment.
Materials and methods
The present study included 35 patients with NTN. The duration of the disease is from 2 to 11 years. All observed patients were undergoing outpatient treatment at the consultative and diagnostic center of the Moscow Regional Research Clinical Institute named after. M.F. Vladimirsky. The age of patients is from 48 to 63 years. The criteria for inclusion in the study were: exacerbation of chronic pain syndrome for no more than 2 weeks.
Standard comprehensive treatment included vitamin therapy, antioxidants, anxiolytics, antidepressants and antiepileptic drugs.
The scientific basis for the use of antidepressants is data on the insufficiency (functional and/or morphological) of antinociceptive systems. It is known that antinociceptive systems exercise inhibitory control of the segmental nociceptive apparatus of the maxillofacial region, located in the caudal part of the nucleus of the spinal tract of the trigeminal nerve. These systems, which include the periaqueductal gray matter, the magnocellular nucleus of the brain stem, the locus coeruleus, etc., are serotonin- and noradrenergic and are involved, along with antinociceptive control, in human emotional reactions. Therefore, the use of drugs with agonistic monoaminergic properties in the treatment of chronic pain is completely justified.
It is possible to use antidepressants of various pharmacological groups: tricyclics (amitriptyline), selective serotonin reuptake inhibitors (fluoxetine), selective serotonin and norepinephrine reuptake inhibitors, melatonin receptor agonists. In our observation, pipofezin (an atypical tricyclic antidepressant) was used at a dose of 75 mg/day.
Antiepileptic drugs were included in the complex pharmacotherapy program for NTN. Depending on the treatment complex used, all patients were divided into 2 groups.
Group 1 (15 people) received carbamazepine (the average daily dose of carbamazepine was 700±230 mg), group 2 (20 people) received pregabalin (Lyrica): 8 patients at a dose of 450 mg/day, 12 – 600 mg/day. The complex pharmacotherapy of patients in both groups included pipofezin 75 mg/day.
In both groups, there were no significant differences in age and gender composition (Table 1).
The observed patients with NTN had a typical course of the disease - an exacerbation began with shooting pains in the projection of one or two teeth, activation of previously existing trigger zones, which were located in the medial part of the face (upper lip, wing of the nose) or in the periodontium of the teeth. In the vast majority of cases, the triggering factor for exacerbation was a sharp change in blood pressure, stress, and temperature changes. Then attacks of intense pain developed. The patients had active trigger zones, irritation of which (washing, eating, shaving) caused a paroxysm of pain.
The patients were examined in two stages - at the initial visit and after 4 weeks. after starting treatment. A comprehensive examination included: neurological examination; Beck Depression Inventory testing; study of pain using a visual analogue 10-point pain scale (VAS) and the McGill pain questionnaire. In order to study the state of nociceptive and antinociceptive systems at the spinal and supraspinal levels, the nociceptive flexor reflex was recorded, which made it possible to quantify the pain threshold in patients with NTN, and exteroceptive suppression of voluntary EMG activity of the masticatory and temporal muscles on both sides.
results
The dynamics of clinical indicators in the observation groups are presented in Table 2.
As follows from Table 2, at the beginning of observation, pain intensity according to VAS in group 1, in which complex treatment included carbamazepine, averaged 6.8 ± 1.3 points, in group 2, in which complex treatment included pregabalin (Lyrica ), – 6.9±1.2 points.
The initial level of depression on the Beck scale before treatment in both groups was significantly high (27 points or more) (p <0.001): in the first group - in 77.3%, in the second - in 72.4% of patients.
The rank level of pain according to the McGill pain questionnaire differed significantly (p<0.01) in the initial groups, without significant differences in the observation groups.
At the second, final stage of observation, in the first group the pain level according to VAS decreased from 6.8 to 2.5 points, in the second - from 6.9 to 1.2 points, respectively (Fig. 1).
A psychometric study at the beginning and at the end of the course of treatment showed that the number of patients with high levels of depression in both groups at the end of the course of treatment decreased due to an increase in the number of those with average values of depression. At the same time, among patients taking pregabalin (Lyrica), the number of patients with high levels of depression decreased significantly compared with the group of patients taking carbamazepine (44.8 and 36.4%, respectively) (Fig. 2).
Results of neurophysiological studies
Nociceptive flexor reflex. When recording the nociceptive flexor reflex (NFR) in patients of both groups 1 and 2, no significant differences in the NFR parameters - pain threshold (PT), reflex threshold (TR) and their ratio (PT/FR) - were found after treatment (p>0.1).
Exteroceptive suppression of voluntary activity of the temporal and masticatory muscles. When recording exteroceptive suppression (ES) of voluntary EMG activity of the masticatory and temporal muscles on both sides in both group 1 and group 2, no significant changes in the latent period (LP) and duration of ES1 were found after treatment (p>0.1) . The main changes identified in patients with NTN after a course of therapy concerned the parameters of late ES2. In both groups of patients after treatment, there was a significant decrease in the LP value and an increase in the duration of the ES2 period of EMG activity of the temporal and masticatory muscles when recording from both the sick and healthy sides, which, however, did not reach the values of these parameters recorded in healthy subjects (p <0.04–0.05).
Table 3 shows the dynamics of parameters of late ES2 voluntary activity of the temporal and masticatory muscles in groups 1 and 2 before and after therapy.
Monitoring of patients in both groups during treatment showed that in the group of patients whose complex treatment included carbamazepine, the following side effects were noted: severe dizziness and ataxia in 12 people, gastrointestinal discomfort (epigastric pain after taking the drug, dyspeptic disorders) – 7 people; in the group of patients taking pregabalin (Lyrica), 3 patients complained of drowsiness during the first 3 days of titration. These undesirable manifestations of therapy with pregabalin (Lyrica) completely regressed during further titration of the drug. Overall, pregabalin (Lyrica) was significantly better tolerated than carbamazepine. One patient refused to take carbamazepine due to poor tolerability of the drug. There were no withdrawals from pregabalin (Lyrica) therapy.
The dynamics of the pain syndrome during treatment were as follows: pain regressed by more than 50% after 2 weeks. drug intake was observed in 12 (60%) patients treated with pregabalin (Lyrica) and in 7 (42.3%) patients treated with carbamazepine. Complete regression of pain after 4 weeks. from the start of taking a therapeutically effective dose of the drug was observed in 9 (60%) patients taking carbamazepine, and in 14 (70%) people treated with pregabalin (Lyrica).
Predictors of treatment effectiveness
In order to determine predictors of the effectiveness of therapy, we divided all patients with NTN who completed the course of treatment into 2 subgroups depending on the degree of pain relief after 4 weeks. from the start of taking an individual effective dose. Subgroup 1 included patients with NTN with complete pain regression - 9 people treated with carbamazepine and 12 people treated with pregabalin (Lyrica). Subgroup 2 included 12 patients with NTN, 6 from each observation group, who experienced a pain reduction of ≥ 50% from the initial value. To identify factors influencing the effectiveness of treatment, we conducted a comparative analysis of patients in these 2 subgroups according to clinical, psychological and neurophysiological indicators before the start of therapy.
Table 4 presents clinical, psychological and neurophysiological indicators according to which patients with NTN of subgroup 1 are significantly different from patients with NTN of subgroup 2.
Based on the analysis, we can conclude that patients who have 4 weeks. treatment, drug remission was achieved (complete pain regression), characterized by:
1) shorter duration of the NTN disease;
2) shorter duration of paroxysms of pain;
3) fewer attacks per day;
4) fewer patients with associated myofascial pain syndrome of the face;
5) lesser degree of depression;
6) lower level of personal anxiety;
7) less pain intensity;
 longer latent period of ES2;
longer latent period of ES2;
9) shorter duration of the ES2 period.
conclusions
The use of antiepileptic drugs in the complex treatment of patients with NTN is effective and safe.
1. Pregabalin (Lyrica) in comparable dosages shows higher analgesic activity, is better tolerated by patients and causes fewer side effects.
2. Long duration of NTN, high (more than 5) frequency of attacks, high levels of depression and anxiety are clinical predictors of an unfavorable prognosis for the effectiveness of pain therapy for NTN.
What diagnostic methods can a doctor prescribe for trigeminal neuritis?
The disease can be caused by various reasons, sometimes very serious (for example, cancer). Diagnosing them is not always easy. Depending on your complaints and information obtained during the examination, the neurologist may prescribe various instrumental studies and laboratory tests.
Magnetic resonance imaging of the head is most often used. This diagnostic method helps to identify pathological changes in the brain characteristic of multiple sclerosis and intracranial tumors.
The doctors of the medical center International Clinic Medica24 adhere to modern current standards - this guarantees that you will be prescribed all the tests necessary in your case, the doctor will not miss anything. At the same time, the coordinating doctor in our clinic will make sure that only truly necessary procedures are prescribed to you, so that you do not overpay for unnecessary things. All types of diagnostics are carried out using our medical center’s own equipment.
The material was prepared by Natalya Yurievna, a neurologist at the international clinic Medica24, Candidate of Medical Sciences Lasch.