Mucosal melanoma is a relatively rare disease and accounts for less than 1% of all melanomas.
These formations have a much more aggressive growth compared to cutaneous forms, are prone to active metastasis to regional and distant sites, and often recur, which causes high mortality rates. The prognosis for mucosal melanomas is poor, with a five-year survival rate of 10–15%.
Melanomas of the mucous membranes of the head and neck region account for half of all mucosal melanomas. They are mainly localized in the projection of the upper respiratory tract, oral cavity and pharynx. Other forms of mucous melanomas belong to the urogenital area. The distribution of tumors by location is presented in the table.
| Localization of melanoma | Prevalence |
| Mucous membrane of the head and neck | 50% |
| Rectal mucosa | 25% |
| Mucous membrane of the female genital area | 20% |
| Mucosa of the digestive tract, conjunctiva and urethra | 5% |
According to scientists, unlike other dermatological cancers, mucosal melanoma does not depend on exposure to ultraviolet radiation. In addition, there are no obvious risk factors for this type of tumor, including family history.
Melanoma of the mucous membranes affects the following organs:
- oral and nasal cavity;
- paranasal sinuses;
- trachea and bronchi;
- lips;
- pharynx;
- esophagus;
- stomach;
- intestines;
- gallbladder;
- anorectal area;
- vulva and vagina;
- urethra and bladder;
- conjunctiva of the eye.
For convenience, mucosal melanomas are sometimes divided into three subgroups:
- melanoma of the gastrointestinal mucosa;
- respiratory;
- genitourinary melanomas.
Given the tendency to early lymphogenous and hematogenous metastasis, it is sometimes difficult to determine whether a mucosal tumor is primary or metastatic. Depending on the location, the tumor will have certain characteristics. For example, primary melanomas of the oral cavity, nose, pharynx, as well as the anorectal and genital areas first develop in a radial direction, increase in area, taking the form of a spot; only then do they gain volume, rising above the surface of the mucosa, and begin to infiltrate the underlying base.
Some mucosal melanomas develop from melanocyte cells that are present in the tissue structure of the organ (lips, nose, oral cavity, anorectal area, etc.). The development of primary melanomas on the mucous membrane of organs where pigment cells are initially absent (trachea, bronchi) can be explained by disorders of tissue embryonic development.
Types and classification
According to the 2021 International Classification of Cancer Stages (TNM), several types of mucosal melanoma are distinguished.
By tumor prevalence:
| T3 | Neoplasms limited to the mucous membrane and lying directly under the soft tissues, regardless of the largest size or thickness |
| T4a | Neoplasms spread to bone structures, deep-lying soft tissues, skin, cartilage |
| Т4b | Tumors spread to the hard muscle, zygomatic bone, cranial nerves, carotid artery |
Based on the presence of regional metastases, tumors are divided into three types:
| Nx | The presence of regional metastases cannot be assessed |
| N0 | There are no regional metastases |
| N1 | Regional metastases are present |
Based on the presence of distant metastases, melanoma of the mucous membranes can be of three types:
| cm0 | No distant metastases were found |
| sM1 | Distant metastases are present |
| рМ1 | Histologically confirmed distant metastases are present |
Some epidemiological aspects (statistics) of skin melanoma
Melanoma occurs approximately 10 times less frequently than skin cancer and accounts for 1–4% of the total structure of human malignant neoplasms. This tumor is one of the most malignant and is characterized by rapid growth and early rapid lymphogenous and hematogenous metastasis.
About half of melanoma cases occur in people aged 30–50 years. It is extremely rare that a tumor can develop in children. Melanoma can develop on the skin of any area of the body, but its favorite localization in women is the lower extremities (lower leg), and in men - the torso (back). In older people, the tumor is somewhat more often localized on the skin of the face.
Over the past ten years, the annual number of cases of skin melanoma in Belarus has increased 1.5 times: from 461 cases in 2001 to 676 in 2010. In general, every 6-8 years the number of patients with melanoma doubles in the world.
In approximately half of the cases, melanoma develops on apparently healthy skin, in other cases - on the site of congenital or acquired pigmented nevi and Dubreuil's melanosis.
Symptoms
The disease is most dangerous because in about a third of cases there are no signs, that is, melanoma is asymptomatic. The other two-thirds of patients note the following first signs of the disease:
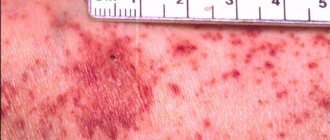
- ulceration of the mucous membrane;
- bleeding in the area affected by the tumor;
- nodular or mocular neoplasm, which can have various shades - reddish, brown, purple, black, gray, white;
- first noted pain caused by wearing orthopedic devices in the oral cavity.
Risk groups and factors predisposing to the development of skin melanoma.
Individuals at increased risk of developing melanoma include:
- with white skin, red hair, blue, gray or green eyes;
- constantly sunburned;
- those who have suffered sunburn and have been exposed to the sun for a long time, especially under the age of 20;
- having close relatives with melanoma (other skin cancer);
- having more than 100 moles on the body or more than 50 before the age of 20;
- having Dubreuil's melanosis (precancerous skin disease).
There are well-known cases of melanoma being diagnosed after injury to a pigmented nevus of the skin (mole). Melanoma often occurs after accidental or intentional (cutting, burning) injury to a mole. Sometimes 1-2 injuries are enough for melanoma to occur.
Trauma to the nevus can be chronic and occur unnoticed. For example, a well-starched shirt collar can injure moles on the neck, and bras can injure moles on the torso. Moles localized on the soles of the feet, palms, and perineum are chronically injured.
The influence of certain hormones on the development and clinical course of melanoma is assumed. Puberty, pregnancy and menopausal changes are regarded as risk factors for the development of melanoma from pigmented nevi.
Genetic predisposition plays a role (familial cases of melanoma).
Diagnostic methods
In order not to miss this disease and to identify it at the earliest possible stage, you need to regularly visit an otolaryngologist and dentist for routine preventive examinations of the mucous membranes of the oral cavity and ENT organs.
The following laboratory and hardware techniques are also used to detect pathology:
- MRI, CT, ultrasound (examination of secondary damage to areas in which regional and distant metastases are located is carried out);
- biopsy, after which the resulting biomaterial is sent to the laboratory for cytological and histological examination;
- determination of the presence of mutations in the BRAF and C-KIT genes.
How is skin melanoma diagnosed?
The most effective method for early detection of skin melanoma is periodic self-examination of the skin. There is a kind of “melanoma alphabet” that describes a number of signs of degeneration of a mole, indicated by the first four letters of the Latin alphabet:
- A (asymmetry) - asymmetry: the shape of “good” moles is often symmetrical;
- B (border irregularity) - the edges of the mole are usually smooth and clear. An uneven, scalloped outline is more characteristic of melanoma;
- C (color) - benign nevi are colored more or less evenly. The unequal color of different parts of the neoplasm is more characteristic of a degenerated mole;
- D (diameter) - the diameter of a mole is more than 6 mm: the larger the mole, the greater the likelihood of its degeneration. Malignant degeneration is indicated by various kinds of changes in a pre-existing mole. It was found that pigmented formations on the skin that regularly changed shape and color turned out to be melanoma 4 times more often than those whose appearance remained unchanged. Therefore, to the first four letters of the “alphabet of melanoma,” a fifth was added;
- E (evolving) - the appearance of any external changes in the mole, which most often are: change in color (decrease or sharp increase in pigmentation); violation or complete absence of skin pattern in the area of the nevus, “varnish” surface or peeling; the appearance of an inflammatory areola around the mole (redness in the form of a corolla); change in configuration along the periphery, blurring the contour of the nevus; an increase in the size of the nevus (especially over the age of 30) and its compaction; itching, burning, tingling in the mole area; the appearance of cracks, ulcerations in the mole area, bleeding; loss of existing hairs on the mole; sudden disappearance of a mole (especially after tanning in the sun or in a solarium).
Very valuable additional clarifying information can be obtained by performing a dermoscopic examination of a pigmented skin tumor, which allows for a visual assessment of the tumor at 10-40x magnification.
Treatment
When treating such a disease, a multidisciplinary, that is, an integrated approach is used. The following treatment methods are used in various combinations:
- surgical intervention in which the primary lesion is removed, and then the issue of the need for cervical lymph node dissection (removal of lymph nodes in the neck) is decided;
- adjuvant radiation therapy;
- adjuvant chemotherapy;
- immunotherapy (if the presence of a mutation in the BRAF and C-KIT genes is confirmed).
Skin melanoma treatment stages 1, 2, 3. Symptoms, signs, metastases, prognosis.
Content:
- General information about melanoma
- What are the different forms of melanoma? Superficial spreading melanoma
- Nodular melanoma
- Malignant lentigo melanoma
- Acral melanoma
- Atypical (dysplastic) nevi
- Primary metastatic melanoma
- Surgical treatment of skin melanoma
Stages of the disease
We suggest you familiarize yourself with the stages of the disease. The staging table is based on the International Cancer Staging (TNM) classification. Each stage is assigned to certain types of melanoma, which we presented above in the tables.
| Stage | T | N | M |
| III | T3 | N0 | M0 |
| IVa | T4a T3-T4a | N0 N1 | M0 |
| IVb | T4b | Any N | M0 |
| IVc | Any T | Any N | M1 |
Provoking factors
The direct causes that influence the formation of gingival melanoma have not been established. However, there are various factors that have a negative impact on soft tissue, which creates a favorable environment for the development of tumor cells on the gums.
Diseases
Chronic and inflammatory gum diseases (periodontitis, papilloma and others) can give rise to malignant neoplasms if not treated in a timely manner.
Damage
People whose gums are regularly exposed to mechanical damage are more likely to develop melanoma. Crowns, dentures and piercings often lead to such damage.
In addition, unprofessional tooth extraction also damages the gums and can lead to inflammation and further development of cancer.
Wrong lifestyle
Smoking, drug addiction and alcoholism are considered provocateurs of various diseases, including gum melanoma.
Poor nutrition
The soft tissue of the gums is very sensitive. Eating too hot or spicy food makes them more vulnerable over time.
If a person has a combination of the above reasons, then the risk of developing gum melanoma increases at least twice.
Forecast
The survival rate of patients who received combination treatment is 4.5-49.2%.
Factors that significantly influence survival prognosis:
- are there regional metastases;
- are there distant metastases;
- what stage – IVa, IVb, IVc;
- invasion (germination) of the neoplasm into the underlying tissues;
- non-radical (incomplete) surgical removal of the primary focus of the disease;
- localization of the tumor (for example, in patients with MSO of the oral cavity, regional metastases appeared in 36.4% of cases, in patients with MSO of the nasal cavity and paranasal sinuses - in 7.8% of cases).
What are the different forms of skin melanoma?
The main clinical forms of melanoma are:
- superficial spreading (39-75%);
- nodal;
- malignant lentigo melanoma;
- acral melanoma.
Superficial spreading melanoma (flat, radially growing melanoma)
The tumor develops equally often both on unchanged skin and from a pigmented nevus. It can be localized on open and closed areas of the skin, mainly on the lower extremities in women and the upper half of the back in men. It is a plaque of irregular configuration with a scalloped outline, areas of regression and discoloration, mosaic coloring, and keratosis on the surface. On average, after a few years, a node appears on the plaque, indicating the transition of horizontal growth to vertical.
Nodular melanoma
Nodular melanoma, accounting for 10-30% of all skin melanomas, is the most aggressive type of tumor. The neoplasm usually appears on unchanged skin. Clinically it is a node, less often a polyp-like formation on the skin. Patients note a rapid, within several months, doubling of the node's volume, its early ulceration and bleeding. The most common localization is the skin of the back, neck, head, and limbs. Histologically, invasion of atypical melanocytes to different depths of the dermis and subcutaneous fat is revealed.
Malignant lentigo melanoma
Melanoma of the lentigo maligna type accounts for about 10-13% of all melanomas and is characterized by a long horizontal growth phase. In typical cases, it occurs in older people on open areas of the skin of the face and neck in the form of black-brown spots or plaques. This type of melanoma is less aggressive than other flat melanomas.
Acral melanoma
Acral melanoma occurs in the nail bed and accounts for about 8% of all skin melanomas. It usually appears as a dark spot under the nail, which makes its timely diagnosis extremely difficult.
Dear patients!
Until about 40 years ago, cutaneous melanoma was a relatively rare disease. However, in recent decades its frequency has increased significantly, and the annual growth rate is up to 5%. Why is melanoma dangerous?
Causes of development and risk factors
Melanoma is one of the types of skin malignant neoplasms that develops from pigment cells - melanocytes that produce melanins, and is characterized by an aggressive, often unpredictable and variable clinical course.
Its most common localization is the skin, much less often - the mucous membrane of the eyes, nasal cavity, mouth, larynx, skin of the external auditory canal, anus, and female external genitalia. This tumor is one of the most severe forms of cancer, disproportionately affecting young people (15-40 years of age), and ranking 6th among all malignant tumors in men and 2nd in women (after cervical cancer) .
It can develop independently, but more often it is “masked” against the background of birthmarks, which does not cause concern for people and creates significant difficulties for doctors in terms of its earliest possible diagnosis. The way this neoplasm develops quickly and is difficult to detect in the initial stages is another danger that often interferes with timely diagnosis. Within 1 year it spreads (metastasizes) to the lymph nodes, and soon through the lymphatic and blood vessels, to almost all organs - bones, brain, liver, lungs.
Causes
The main modern theory of the occurrence and mechanism of development of melanoma is molecular genetic. In accordance with it, in normal cells DNA damage occurs in the form of gene mutations, changes in the number of genes, chromosomal rearrangements (aberrations), violations of chromosomal integrity, and the DNA enzyme system. Such cells become capable of tumor growth, unlimited reproduction and rapid metastasis.
Such disorders are caused or provoked by damaging risk factors of an exogenous or endogenous nature, as well as their combined effects.
Exogenous risk factors:
Chemical, physical or biological environmental agents that have a direct effect on the skin.
Physical risk factors:
- Ultraviolet spectrum of solar radiation. .
- Increased background of ionizing radiation.
- Electromagnetic radiation - tumor is more common among people professionally associated with telecommunications equipment and the electronics industry.
- Mechanical trauma to birthmarks, regardless of its frequency, is a high risk. It is not entirely clear whether it is the cause or the trigger, but this factor accompanies 30-85% of melanoma cases.
Chemical factors are important mainly among those working in the petrochemical, coal or pharmaceutical industries, as well as in the production of rubber, plastics, vinyl and polyvinyl chloride, and aromatic dyes.
Of the biological factors, nutritional characteristics are of greatest importance. High daily intake of animal proteins and fats, low intake of fresh fruits and vegetables high in vitamins A and C.
With regard to the systematic consumption of alcoholic beverages, it is theoretically assumed that they can provoke the growth of melanomas, but there is no practical evidence of this. It has been precisely proven that there is no connection between the consumption of drinks containing caffeine (strong tea, coffee) and malignant neoplasms. Therefore, nutrition for skin melanoma should be balanced mainly with products of plant origin, especially fruits and vegetables, and contain a rich amount of vitamins and antioxidants (blueberries, green tea, apricots, etc.).
Taking oral contraceptives, as well as estrogen drugs prescribed for the treatment of menstrual irregularities and autonomic disorders accompanying menopause. Their influence on the development of melanoma remains only a guess, since no clear relationship can be traced. Endogenous risk factors are divided into two groups, one of which consists of factors that are a biological feature of the body:
- low degree of pigmentation - white skin, blue and light eyes, red or blond hair, a large number of freckles, especially pink ones, or a tendency to have them;
- hereditary (family) predisposition - what matters is mainly the disease of melanoma in the parents; the risk increases if the mother was ill or there were more than two people with melanoma in the family;
- anthropometric data - a higher risk of its development in people with a skin area of more than 1.86 m2;
- endocrine disorders - high levels of sex hormones, especially estrogens, and melanostimulating hormone (melatonin), produced in the middle and intermediate lobes of the pituitary gland; the decrease in their production after the age of 50 coincides with a decrease in the incidence of melanoma, although some authors, on the contrary, indicate an increase in its frequency in older age;
- immunodeficiency states;
- pregnancy and lactation, which stimulate the transformation of pigmented nevi into melanoma; this is typical mainly for women with a late first pregnancy (after the age of 31), and pregnancy with a large fetus.
The second group is nevi, which are skin changes of a pathological nature and are characterized by the highest degree of probability of degeneration into melanoma, and are also its predecessors. These are benign formations consisting of pigment cells (melanocytes) of varying degrees of maturity (differentiation), located in varying numbers in different layers of the skin. A congenital nevus is called a birthmark, but in everyday life all formations of this type (congenital and acquired) are called birthmarks. The greatest risk is represented by black or dark brown pigmented nevi measuring 15 mm or more.
Melanoma symptoms
At the initial stages of the development of a malignant tumor on healthy skin, and even more so against the background of a nevus, there are few obvious visual differences between them. Benign birthmarks are characterized by:
- Symmetrical shape.
- Smooth, even outlines.
- Uniform pigmentation, giving the formation a color ranging from yellow to brown and even sometimes black.
- A flat surface that is flush with the surface of the surrounding skin or slightly evenly raised above it.
- No increase in size or slight growth over a long period of time.
What does melanoma look like?
It may take the form of a flat pigmented or non-pigmented spot with a slight elevation, round, polygonal, oval or irregular in shape with a diameter of more than 6 mm. It can maintain a smooth shiny surface for a long time, on which small ulcerations, unevenness, and bleeding subsequently occur with minor trauma.
Pigmentation is often uneven, but more intense in the central part, sometimes with a characteristic rim of black color around the base. The color of the entire neoplasm can be brown, black with a bluish tint, purple, variegated in the form of individual unevenly distributed spots.
In some cases, it takes on the appearance of overgrown papillomas, resembling a “cauliflower”, or the shape of a mushroom on a wide base or on a stalk. Near the melanoma, additional separate lesions (“satellites”) sometimes appear or merge with the main tumor. Occasionally, the tumor manifests itself as limited redness, which turns into a permanent ulcer, the bottom of which is filled with growths. When developing against the background of a birthmark, a malignant tumor can develop on its periphery, forming an asymmetric formation
Knowledge of reliable and significant symptoms of the transition of benign formations to an active state is of great importance. How to recognize a malignant formation and the moment of transformation of a birthmark into it? Early signs are as follows:
- An increase in the planar dimensions of a previously unchanged or very slowly enlarging mole, or the rapid growth of a newly emerging nevus.
- Changing the shape or outline of a pre-existing formation. The appearance of compactions or asymmetry of contours in any part of it.
- Change in color or disappearance of uniform coloring of an existing or acquired birthmark.
- Change in intensity (increase or decrease) of pigmentation.
- The appearance of unusual sensations - itching, tingling, burning, “bloating.”
- The appearance of redness around the birthmark in the form of a corolla.
- Disappearance of hair from the surface of the formation, if any, disappearance of the skin pattern.
- The appearance of cracks, peeling and bleeding with minor injuries (light friction with clothing) or even without them, as well as growths like papilloma.
The presence of one of these symptoms, and even more so their combination, is a reason for the patient to contact a specialized oncology treatment and prevention facility to carry out differential diagnosis and decide how to treat melanoma, which depends on its type and stage of development.
Diagnosis of a malignant tumor is carried out mainly through:
- Familiarization with the patient’s complaints, clarification of the nature of changes in the “suspicious” formation, its visual examination, examination of the entire patient in order to count the number of birthmarks, identify those that are different among them and further study them.
- Conducting general clinical examinations of blood and urine.
- Hardware dermatoscopy, which allows you to examine the neoplasm in the skin layers, magnified several dozen times (from 10 to 40), and make a fairly accurate conclusion about its nature and boundaries according to the relevant diagnostic criteria.
- Ultrasound examination of the abdominal organs, computed and magnetic resonance imaging of the spinal cord and brain, radiography of the chest organs, allowing to determine the spread and presence of metastases in other organs.
- Cytological examination of a smear (in the presence of ulcerations) and/or material obtained by puncture of a lymph node (in rare cases). Sometimes examination of punctate from an enlarged lymph node allows one to diagnose the presence of the disease in the apparent absence of a primary tumor.
The main method is surgical knife, laser or radio wave excision of the tumor. In the presence of metastatic foci, a combination of surgery with chemotherapy and immunotherapy is used.
How is a malignant tumor removed?
If tumor metastases are not detected, the affected area of skin on the body and limbs is excised at a distance of 3-5 cm from its visible edge, along with subcutaneous fatty tissue, aponeurosis or muscle fascia. When localized on the skin of the face, hands and near the natural opening - at a distance of 2-3 cm, on the fingers (subungual form) - amputation or disarticulation is carried out, on the upper and middle parts of the auricle - removal of the latter.
In the presence of ulcerations of a tumor that grows into the dermis, as well as the presence of metastases in the nearest (“duty”) lymph node, the entire “package” of lymph nodes with subcutaneous tissue is simultaneously removed.
Treatment after surgery
Therapy is carried out mainly in the presence of metastases or at least when such a possibility is suspected. For these purposes, chemotherapy, immunotherapy, or a combination thereof is used. The most common drugs for treatment are intravenous or intramuscular administration of Cyclophosphamide, Imidazolecarboxamide, Cisplatin, Dacarbamazine, Carmustine. More often, combined treatment with these drugs is carried out with Vinblastine and Metatrixate, as well as with immunotherapy drugs - Interleukin-2 or Interferon-alpha. This combination helps prevent relapses.
Melanoma is characterized by low sensitivity to radioactive radiation. Therefore, radiation therapy is carried out only as a symptomatic or palliative effect, as well as in cases where the patient refuses radical surgery. In addition, it is sometimes used as preoperative preparation and after surgery.
After radical treatment, all patients are subject to constant medical examination in order to timely detect and treat recurrent cancer.
Dermatologist Nazarova N.G.