Implantation is a method of restoring teeth in which a titanium pin is screwed into place of the missing root. Dental implantation is the only procedure today that restores the functionality and aesthetics of teeth to the fullest.
However, it is worth keeping in mind that implantation is a surgical intervention and, like any operation, has its consequences. Sometimes they are minor and go away on their own. In some cases, the problem must be solved by a doctor.
Complications after dental implantation are conventionally divided into 3 types:
- Operating
- Postoperative early
- Postoperative late
What can happen during surgery
No matter how expensive and high-quality implants are, complications during surgery depend on the qualifications of the implantologist. This is why choosing a doctor is so important. Experienced doctors practically never have misfires in the form of:
- Bleeding
due to vessel damage
Bleeding may be associated with increased blood pressure and poor blood clotting. However, in the vast majority of cases, vessel rupture occurs due to surgeon error.
- Perforation of the maxillary sinus
In the upper jaw there is little bone for installation; it often has to be replanted (sinus lift). When implanting upper teeth, it is easy for the doctor to make a mistake and drill a hole that is too deep. 3D modeling and surgical guides, coupled with the surgeon's experience, significantly reduce such cases.
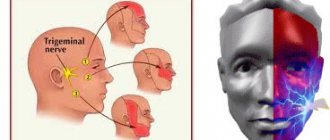
- Nerve injury
When working on the lower jaw, there is a possibility of touching the alveolar, mental or lingual nerve. This leads to numbness. This is why implantologists insist on performing a CT scan before surgery, this helps to make accurate measurements in the area where the pin is being implanted.
Alveolar wall
The result of an incorrectly selected implant size.
Modern technologies: 3D modeling, surgical templates, CT and orthopantomogram virtually eliminate operational errors.
Problems during the second surgical stage
The second stage of dental implantation involves:
- opening the implant (to do this, the doctor cuts the gum above it);
- removing the plug;
- installation of a gum former.
Due to disorders of bone regeneration, the intraosseous element is twisted, and when implanting teeth in the upper jaw, it is pushed into the maxillary sinus. This complication is prevented at the stage of formation of bone tissue around the implant - during the period of osseointegration, CT is periodically performed to monitor the formation of bone structures.
There are opposite situations when the top of the implant is overgrown with bone tissue. This process is not considered a complication and does not have a special impact on the implantation process. The doctor cuts the periosteum and removes excess with a saw to properly install the healing abutment.
Problems after implantation - what you shouldn’t be afraid of
After any surgical intervention, the body needs time to recover. A reaction to surgery may (but does not necessarily) include the following symptoms:
- Pain
in the jaw after the anesthesia wears off.
They disappear in 2-3 days
, maximum
in a week
, gradually weakening. - Moderate bleeding 2-3 hours
after surgery. Sometimes, saliva may be pink for 2-3 days, but there is no bleeding as such. - Edema
. They may increase during the first 3 days after surgery, but then subside. - Temperature increase
.
For 2-3 days,
the temperature can rise to
37.3
degrees, but overall health remains normal. - Loss of sensation
. Recovers on its own in a short period of time.
Complications during prosthetics
- An increase in the temperature of the implant at the time of preparation of its head.
- Incorrect placement of the implant head.
- Incorrect installation of dentures.
To prevent the implant from heating up during the preparation of the heads, it is necessary to constantly irrigate the preparation area and the bur itself.
If the head of the implant is not connected tightly enough to the intraosseous element, this inevitably leads to overload of the remaining supports of the prosthesis and becomes a site of accumulation of tissue fluid and microbial plaque, which is fraught with the occurrence of peri-implantitis.
Errors in the installation of conditionally removable dentures are, in fact, uneven tightening of the screws that secure the denture, and, as a result, overloading of some implants and loose fit of the denture to the heads of other implants, on which microbial plaque accumulates. This is dangerous due to the occurrence of peri-imlantitis.
Errors in installing a combined prosthesis may include untimely tightening of the screws when the cement has already hardened. The screws must be screwed in before the cement sets, because the hardened cement may crack.
Early complications after implant installation
The success of any implantation depends on many factors, which cannot be taken into account. These include the individual characteristics of the body, the reaction to intervention, the presence of contraindications and compliance with recommendations. Yes, modern implants have a high survival rate, up to 99%
, but there is always that 1% that will cause complications. It could be:
Early peri-implantitis
This is an inflammation of the tissues adjacent to the implant. This leads to a pocket forming between the pin and the bone and tissue loss.
During the operation, the outer coverings of the oral cavity, which protect the body from infections, are damaged. Bacteria can enter a poorly treated wound. The same thing happens if oral hygiene is insufficient after surgery. Inflammation can be caused by overheating of tissues during implantation.
In the initial stages, peri-implantitis is treatable. In advanced cases, the pin is removed.
Implant rejection
A few days after implantation, the patient notices mobility of the pin, which increases. The gums turn red and swell. Possible fistula formation. The x-ray shows that the bone is being destroyed. This causes mobility of the implant. It will have to be removed. Rejection is caused by bacteria that provoke purulent inflammation of the bone, or overheating of the bone during surgery.
Dental implant systems with minimal risk
There is a huge variety of implants, differing in many ways.
Dental systems with an impeccable reputation are produced in Switzerland, Germany, and Israel.
To protect yourself as much as possible when choosing implants, you need to consider the following criteria :
- structures must be made of highly purified titanium ;
- the surface of the implant must have macro- and microthreads ;
- the presence of a conical connection between the implant and the abutment;
- lifetime warranty on the system;
- time of existence of the manufacturing company in the dental market.
Long-term consequences after dental implantation
If early complications depend more on the doctor’s mistakes, then later ones are the patient’s responsibility. The vast majority of problems after dental implantation occur as a result of insufficient oral hygiene:
- Mucositis and hyperplasia.
Inflammation of the gingival cuff as a result of plaque formation on the head of the implant. The gums turn red, swell, and ulcers form on it. Plaque must be removed and care taken more thoroughly. - Late peri-implantitis.
Reason: poor hygiene and constant traumatic exposure. If your bone density is low, additional tissue will need to be grafted. - Sinusitis.
Inflammation of the maxillary sinuses can be caused by peri-implantitis. If the pin is mobile and there are signs of inflammation, the implant is removed and sinusitis is treated. If these signs are not present, then sinusitis is treated without removing the implant.
Average cost of treatment in Moscow
| Service | price, rub. |
| Consultation with specialists: | |
| dentist | 600 |
| periodontist | 740 |
| implantologist | 820 |
| Services for the treatment of complications: | |
| laser therapy of the gum mucosa | 490 |
| periodontal applications in the area of one tooth | 370 |
| removal of dental plaque in the area of one tooth | 180 |
| implantation of osteoconductive material in the area of one tooth | 10900 |
| implantation of a protective membrane | 12900 |
| application of a protective periodontal bandage | 400 |
| implant removal | 6900 |
The cost of treating complications after implant placement varies depending on the severity of the consequences , extent of spread and treatment methods .
Treatment
An x-ray allows the dentist to understand exactly what the problem is. Mostly, complications are caused by inflammatory processes. Anti-inflammatory therapy, antiseptic surface treatment, and hygienic care are carried out.
In case of peri-implantitis, inflamed tissue is removed, the pin is cleaned and treated with an antiseptic.
In some cases, complications after dental implantation require removal of the post. For example, if the implant breaks, it is rejected, or treatment of inflammatory processes is not successful.
The implant is removed by carefully twisting it out of the bone, trying to minimize trauma to surrounding tissue.
The issue of re-implantation is considered in each case separately. Most often, a two-stage protocol is impossible without bone grafting. But with the one-step method, you can do without it. In any case, you will have to wait until the inflamed tissues recover. However, it should not be delayed to avoid bone loss.
The decision to re-implant after removal of a dental implant must be made by the doctor. It takes into account all the factors necessary for the success of the operation. If rejection is caused by biological reasons, low immunity, smoking, then the positive result of re-implantation is in doubt and it is better to use alternative prosthetic methods.
The success rate of dental implantation as a treatment option for restoring missing teeth in Russia and the world has increased significantly in recent years. The risks and complications of dental implantation remain on the agenda, although implant systems and various surgical treatment methods are constantly being improved.
Dental implants today are designed to suit individual anatomy and different bone types. Intraosseous implants fail for many reasons. This review article discusses various causes of implant failure and contributing risk factors.
A better understanding of the factors responsible for dental implant failure will allow more informed clinical decisions to be made and may expand the capabilities of dental implant dentistry.
Replacing missing teeth with titanium dental implants is currently the gold standard in dental rehabilitation. Various statistically analyzed factors associated with dental implant failure include age and gender, smoking, systemic diseases, maxillary implant placement, bone quantity and quality, and implant surface characteristics.
Immunological and genetic factors have also been reported to be associated with early implant failure. Periodontitis and smoking are associated with higher rates of treatment failure. Thus, smoking reduces blood supply to local tissues, interferes with healing and chemotaxis, and significantly weakens systemic immunity. The implant failure rate is known to be 11% for smokers compared to 5% for non-smokers.
Mellado-Valero et al found a greater risk of treatment failure in diabetic patients within one year of exercise. Dental implant failure is more likely to occur in pre-irradiated bone and after excessive increase in bone temperature during placement, resulting in necrosis of the supporting tissue around the implant.
Age as a risk factor
Patient age is considered one of the most important predictors of dental implant success. Older patients are more likely to have severe systemic disease, poor bone health, and potentially longer healing times.
A number of researchers believe that older age increases the risk of implant failure, with patients over 60 years of age having poor treatment outcomes for two reasons. Brocard et al examined cumulative success rates in a long-term study and concluded that patients over 60 years of age had poorer implant survival.
Dental implant sinking continues throughout adult life and its rate varies with age. This process is much more noticeable in the second and third decades of life compared to the fourth and fifth.
The age at which growth is completed also varies widely from patient to patient. Typically, the growth spurt occurs at age 12 for girls and age 14 for boys, but this can vary by as much as 6 years. Thus, when planning for dental implants for a child, this potentially problematic age period extends from 9 to 15 years for girls and from 11 to 17 years for boys.
Displacement of the teeth of the upper and lower jaw
Spontaneous displacement of teeth during the stepped dentition phase is a well-studied phenomenon. Between 10 and 21 years of age, there is a mesial displacement of the teeth in the lateral segment of the jaw (from the canine to the first molar) of approximately 5 mm. The displacement of the incisors on the cheek side reaches 2.5 mm, which can lead to loss of space in the arch and compaction.
A dental implant does not move teeth. Thus, the implant can stop this process, leading to asymmetry. The implant in the front cannot follow the teeth and over time this misalignment will become more pronounced. Depending on facial growth patterns and subsequent tooth eruption, vertical changes may still occur after puberty, although at a slower rate than during the active growth phase.
Hygiene and oral care
The accumulation of bacterial plaque leads to gingivitis, periodontitis and peri-implantitis. In addition, the presence of any symptoms of infection, radiographic evidence of peri-implant bone loss or neuropathy, decreased vascularity in combination with parallel oriented collagen fibers may indicate certain complications or implant failure.
This can be dealt with using interdental interproximal brushes (brushes) penetrating 3 mm into the gingival sulcus or pocket. The problem also requires evaluation of the prosthetic component for plaque and calculus, implant support stability, peri-implant tissue margin, implant body, and radiographs every 12 to 18 months.
Some other clinical conditions are associated with oral lichen planus, bad habits, opposition to traditional flap surgery or piezoelectric surgery, dental health, and the harmful effects of smoking.
The role of bruxism in dental implantation
Glauser et al analyzed a group of 41 patients who received 127 immediate loading implants. Their results showed that patients with bruxism experienced significantly more implant loss compared to patients without parafunction (41% vs. 12%).
The higher failure rate in this group is associated with uncontrolled functional loading of the implant, which leads to micromovements above a critical limit with subsequent fibrous encapsulation of the implant instead of osseointegration. It has been suggested that early or immediate loading is not detrimental to osseointegration unless excessive micromotion occurs at the bone-implant interface during the healing phase.
Smoking as a risk factor
Smoking has a significant negative impact on oral health, nutritional status, and the overall health of the immune system. Dental implants have a much lower survival rate in smokers.
At the cellular level, smoking reduces the activity of leukocytes, causes a decrease in the rate of chemotactic migration and low phagocytic activity, which leads to low overall resistance to infections and delayed wound healing.
Smoking also reduces the absorption of calcium from the digestive tract. Smoking affects the process of osseointegration by reducing blood flow due to increased peripheral resistance and platelet aggregation.
Toxic substances from tobacco smoke, such as carbon monoxide and cyanide, slow down the ability to heal wounds and, together with nicotine, suppress the rate of cell proliferation. Tobacco directly inhibits osteoblast function by impairing osseointegration.
Strietzel et al reported that smoking negatively affects the prognosis of dental implant placement with or without augmentation. Studies show significant marginal bone uptake in smokers compared to non-smokers.
penetration
into the sinus
Immediate placement of a dental implant into unstable residual bone may result in penetration of the implant or graft into the maxillary sinus, affecting the natural movement of cilia in the maxillary sinus and mastication (<5 mm of bone).
This problem can be addressed surgically using a variety of approaches, including intraoral, endoscopic, transnasal, and maxillary bone reconstruction.
Bisphosphonate-associated osteonecrosis
Bisphosphonates work in sites of active bone remodeling, such as the jaw, by promoting surgical trauma to the alveolar bone during implantation and further increasing postoperative drug accumulation at the implantation site.
Bisphosphonates disrupt bone metabolism and reduce the resistance of the bones around the implant to oral flora, causing an increased risk of developing peri-implantitis.
Trauma to an adjacent tooth
Placing an implant in the wrong axis or inserting an implant that is too large can cause trauma to the adjacent tooth, leading to tooth loss.
Extended roots and excessive mesiodistal inclination wear away the implant area and prevent ideal implant placement. Correct interpretation of the radiograph using a 5 mm deep guide pin facilitates angular correction of the osteotomy.
As an alternative method, differences between the apical and ridge interdental spaces due to mesial or distal root inclination can be corrected orthodontically.
Peri-implantitis
Peri-implantitis is a progressive inflammatory condition that affects the tissue surrounding an osseointegrated implant, leading to loss of supporting bone and implant failure. The complication is characterized by bleeding, suppuration, increased probing depth of the pockets, implant mobility, and radiographic bone loss.
This inflammatory process is more intense and spreads deeper and faster around the dental implant compared to inflammation around an adjacent natural tooth. Cocci and subgingival microflora causing peri-implantitis are believed to be the most important causes of dental implant failure.
Mild laser irradiation is effective in removing bacterial pathogens that cause peri-implantitis. Systemic antibiotics against gram-negative anaerobes alter the oral microbial composition and clinically improve the condition in the long term.
Topical delivery devices such as Actisite, whose fibers contain polymer tetracycline hydrochloric acid, can be used to significantly reduce the total number of anaerobic bacteria.
Irradiated bone
Radiation therapy, along with surgical removal, is the treatment protocol used for malignant tumors of the craniofacial region. This increases the risk of complications from dental implantation.
The success rate of installing dental implants in irradiated bone is 70%. Hyperbaric oxygen therapy administered to irradiated patients prior to implant therapy increases the likelihood of successful implant placement.
Hyperglycemia as a risk factor
Hyperglycemia can also affect the osseointegration of dental implants, predisposing to the development of complications. Hyperglycemia alters the functioning of parathyroid hormone, which helps regulate phosphorus and calcium metabolism and inhibits osteoblast differentiation. It affects the bone matrix, its components, as well as adhesion, growth and accumulation of extracellular matrix.
Normal glucose levels after insulin treatment initiate bone matrix growth and osteoid formation. Hyperglycemia can reduce bone recovery by 40% after circumferential osteotomy.
Effective insulin treatment normalizes this recovery index, indicating that poor bone healing is largely associated with poor diabetes control. Failures that occur after the second phase of the operation and within one year of functional load are associated with microangiopathy, which occurs as a complication of diabetes. This may compromise the vascularization of the flap, cause soft tissue infection, and delay healing.
Osteoporosis and complications of dental implantation
Impaired osseointegration in patients with osteoporosis occurs due to decreased bone mass and density. However, osteoporosis does not necessarily affect the bones of the upper and lower jaw if it is diagnosed in another part of the skeleton.
Intravenous use of bisphosphonates is associated with osteonecrosis of the jaw. Foreign scientific literature reports 63 cases of osteonecrosis of the jaw in patients with cancer or osteoporosis. Dental implantation in patients taking bisphosphonates for a long time should be performed with caution.
Corticosteroid therapy
Patients receiving systemic corticosteroid therapy are more likely to experience decreased bone density, increased epithelial fragility, and immune suppression, which in turn leads to impaired osseointegration of the dental implant.
In case of long-term use of corticosteroids, the drug intervention and the degree of adrenal suppression must be taken into account.
Immunodeficiency
Immunocompromised patients are more susceptible to infections and impaired tissue repair. According to new research, the installation of dental implants is successfully performed in patients with a stable immune status, including HIV-positive patients with sufficient CD4 + cell counts and the use of antiviral drugs.
Bleeding disorders
Uncontrolled bleeding can be caused by platelet disorders, clotting factor deficiencies, and the use of anticoagulant drugs such as aspirin and warfarin. It is associated with platelet deficiency to levels <50,000/mm3.
The most life-threatening complication of dental implant placement in these patients is upper airway obstruction, which should be taken into account during treatment.
Cardiovascular diseases
Cardiovascular disease interferes with the healing process and osseointegration, leading to decreased fibroblast activity, impaired macrophage function, and decreased collagen synthesis. These pathologies include hypertension, atherosclerosis and congestive heart failure. Cardiovascular disease does not have a significant impact on the long-term success of dental implant surgery.
Organ transplantation (heart/liver/kidney)
Organ transplant patients often undergo long-term treatment with immunosuppressive drugs to prevent transplant rejection.
Cyclosporine A is usually prescribed in combination with steroids (anti-inflammatory). Cyclosporine may have a negative effect on mechanical fixation and peri-implant bone healing.
Conclusion
There is currently an urgent need to increase our awareness of potential risk factors that may affect the success of dental implant surgery. This can be achieved through ongoing dental education programs and seminars.
New research provides an inexhaustible source of objective information for specialists, and modern ideas about the limitations of this procedure change quite quickly and require constant attention.
Regular assessment of theoretical and practical knowledge in this area is mandatory to achieve more stable predictable treatment results and minimize the risks and complications of dental implantation.
Main features of the technique
Dental implantation is an innovative technology for implanting artificial roots into the upper or lower jaw arch. The design consists of a titanium screw and abutment. Implants (supports) are used to further fix the crowns. The abutment is installed inside the titanium screw after its complete healing. This element is the outer part of the tooth structure. It 100% imitates a ground tooth prepared for prosthetics.
The production of implants and the process of dental implantation itself is carried out today in many countries around the world. Popular designs for dental implantation are produced in America, Germany, Switzerland, Korea and other countries. The technique is also in demand in Russia. Experienced doctors can perform implantation for you. Just contact the clinic and let us know your desire.
Modern dentistry allows all manipulations to be carried out without pain and discomfort for the patient and even within a limited time frame.
The main advantages of dental implantation include:
maintaining the integrity of adjacent elements of the dentition;- better cosmetic effect (compared to standard prosthetics);
- long service life of the structures used;
- stimulation of osteosynthesis, prevention of premature wrinkles.
The designs produced under well-known brands allow you to chew any food, communicate and smile without embarrassment, and lead a normal lifestyle.
Dental implantation is performed when:
- one- and two-sided end defects;
- the absence of one or all teeth on the upper and lower jaw;
- atrophy of the alveolar processes;
- inability to use removable dentures;
- diseases of the digestive system due to insufficient chewing of food.
The technique is relevant for patients aged 18 to 70 years.
Question answer:
I don’t have enough bone tissue, they suggested basal implantation. What complications are possible?
Basal implantation is a branch of surgical dentistry, which involves restoring the dentition without replenishing bone tissue deficiency. Implants are installed even if there is a lack of cancellous bone. This reduces the number of necessary surgical procedures and shortens the treatment time, but the method is not confirmed by positive results of long-term data and has many disadvantages: traumatism - elongated titanium rods are used, which are installed in the deep layers of the jaw bone; difficult rehabilitation - long, accompanied by swelling and pain; used when 3 or more teeth are lost - implants are installed at an angle and can damage the roots of adjacent teeth; the service life of implants has not been confirmed; the 2-year rejection rate is about 40%; rejection occurs with exfoliation of bone tissue; low aesthetic result - it is impossible to make dentures that look like natural teeth; limits the possibilities of prosthetics using other methods.
Levin Dmitry Valerievich
Maxillofacial surgeon, chief physician of the Center
Service life of structures
Experts guarantee a long period of operation of implants.
To do this, you need to follow a few simple recommendations:
- keep the oral cavity in satisfactory condition. Visit the dental office twice a year;
- do not overload the structures.
Provided that all protocols are followed during implantation and manufacturing of orthopedic structures, the service life of the products reaches 25 years.
Implantation is the most advanced method of rehabilitation of lost functions of the masticatory apparatus. Despite the maximum automation of processes at all stages, the quality of treatment largely depends on the professionalism of the doctor. The choice of a clinic and a doctor must be approached with all responsibility.
Results of dental implantation
Today, the vast majority of procedures are successful, but in some cases the implant may not fuse well with the bone. Smoking, for example, contributes to implant loosening and other serious complications.
If the implant becomes loose, the implant is removed, the bone is thoroughly cleaned, and you can try the treatment again after 2-3 months of recovery.
To prevent complications, doctors recommend:
- Oral hygiene
: Just like natural teeth, crowns need to be kept clean. Specially designed brushes for thorough cleaning of the interdental space will help avoid the accumulation of bacteria and inflammation.
- Regular visits to the dentist
: To prevent infections, preserve implants and receive timely care, visit your doctor every six months.
- Avoiding bad habits
: in addition to smoking, which contributes to loosening of the implant, you should not chew very hard food (caramel) or use new teeth for other purposes. Let's say, for opening bottles.
Take care of your health and return to the surgeon as rarely as possible!
Orthopedic stage
At this stage, the anatomical structure of the teeth and chewing function are completely restored. The implantologist and the orthopedist begin close collaboration to create an artificial dental unit that best matches the characteristics of the patient’s dental system.
Impressions are taken using an impression tray. The resulting impression becomes the basis for creating an artificial crown. Procedure to complete:
- the shaper is removed;
- a transfer is screwed into the implant;
- select the required spoon size;
- the first layer of casting material is placed in it;
- a second layer of material is applied around the transfer;
- the spoon is positioned in the mouth;
- then removed and transferred to the dental department;
- A working model of the prosthesis is made.
Repeated fittings take place, during which the product can be adjusted. Typically, the crown production process lasts 3–4 weeks.
Next comes the fixation of the structure - this process depends on the type of crown selected. To install a single version and small bridges, a special adhesive material is used. Fixation of structures with partial or complete edentia is performed using locks built into the prosthesis. A cheap option is installation by screwing screws into the implants through holes in the crown, masked by composite material.
In what cases should implantation be postponed or abandoned?
Relative contraindications to dental implantation are:
- acute infections;
- diseases of the skeletal system;
- pregnancy in the 1st, 3rd trimester;
- pathologies of the immune system;
- cancer and other serious diseases.
Dental implantation may be delayed due to:
- inflammatory processes in the oral cavity;
- periodontal diseases;
- malocclusion;
- bruxism, etc.
Your doctor will tell you about all indications and contraindications.
He will also select the optimal option for dental implantation.
In what cases can complications arise?
The use of innovative technologies in dental implantation, equipment and instruments minimizes the possibility of making mistakes during treatment.
However, errors do occur. They usually occur if the doctor has recently performed implantation. That is why it is very important to contact experienced specialists.
So, the following errors are usually noted:
- violations of surgical protocol;
- non-compliance with the rules of asepsis and antiseptics;
- lack of consideration of the patient’s anatomical features;
- carelessness when working with fabrics.
Errors can occur when choosing an anesthetic and in other cases.
All of these errors often provoke a number of complications.
Among them:
- swelling of tissues;
- soreness;
- implant mobility;
- exposure of the cervical area of the tooth;
- fracture or loss of a dental element.
Implantation: main options
The following options for dental implantation exist:
- intramucosal - with the introduction of push-button elements into the mucous membrane of the gums;
- submucosal - with the installation of a magnet and a removable denture on it;
- subperiosteal - with integration of a metal frame with supporting parts;
- endodonto-endosseous - with the introduction of a pin into the bone tissue (with tooth mobility);
- intraosseous - with the introduction of non-removable dental implants fixed in bone tissue;
- transosseous - in which the implant penetrates the entire jaw arch and is attached to its base.
Dental implantation can also be:
- one-stage – with the introduction of non-removable implants;
- two-stage – using collapsible structures;
- direct – in which the implant is inserted into the socket of a newly extracted tooth without incisions or sutures;
- sharpened - in which several months pass from the moment of tooth extraction to implantation (necessary for healing of the hole).