Endodontics is a field of dentistry that specializes in the study and treatment of diseases of the root canals of teeth, in particular chronic pulpitis and periodontitis.
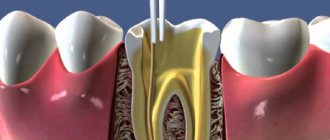
Pulp is the soft tissue that fills the cavities of both the crown of a tooth and its root canals. The root canals of a tooth end in an almost imperceptible apical foramen, which is located at the apex of the tooth root.
Pulpitis is an inflammatory process of the pulp. It is caused by bacteria from the cavity affected by caries entering the crown pulp, and subsequently into the root pulp. Pulpitis can be caused by trauma, as well as diseases of the gums or periodontal pockets.
Stages of endodontic treatment:
- Organization of access to the root canal of the tooth.
- Removing pulp from the canal.
- Filling the canal with a material that helps seal it (filling).
Endodontic dental treatment can be primary and secondary (repeated).
Carrying out treatment
All manipulations are performed under local anesthesia. The tooth to be treated is prepared, the pulp affected by caries is removed, after which the canals are cleaned to ensure easy access for dental instruments.
The root canals are mechanically processed and chemically disinfected.
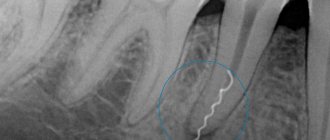
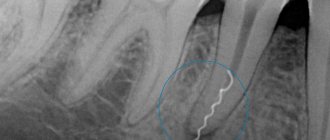
For mechanical treatment of root canals, special tools are used - files; they are somewhat similar to a needle with a rough surface resembling a saw. Files vary in size, length and taper. Since the root canal must be processed along its entire length with files, up to the apical foramen (but in no case beyond it), it is extremely important to find out its length. To do this, the dentist places files into the root canals and takes an x-ray.
After this, chemical disinfection is carried out by irrigating the root canals with special needles.
When the canals are completely dry, you can begin filling them. Gutta-percha and pastes are most often used for this purpose. Gutta-percha is a cone-shaped rubber rod that is coated with a paste and placed into the root canal. Then a temporary filling is placed on the tooth, which is replaced with a permanent one at the next appointment.
| Tooth destroyed by caries, inflamed pulp | Mechanical treatment of root canals with a file tool | Filling canals with gutta-percha, filling a tooth with a temporary and then permanent filling | For further protection, the tooth can be covered with a porcelain crown. |
Material and methods
The first stage was a laboratory study to determine the physical and mechanical properties of samples of dual-curing nanocomposite material LuxaCore Z-Dual and dual-curing composite material LuxaCore-Dual (Table 1). According to GOST 31574–2012, 88 samples were manufactured and tested, 22 for each type of test.
Table 1. Characteristics of materials used in the study (according to manufacturers)
Bending testing of material samples was carried out in a Zwick/Roell testing machine at a crosshead speed of 0.75±0.25 mm/min with a maximum load of 5000 N. The samples were loaded until they failed. To determine the diametric tensile strength of material samples, they were subjected to a uniform compressive force in a Zwick/Roell Z 1010 testing machine until complete destruction at a crosshead speed of 10±0.25 mm/min. The load was always applied to the sample along its longitudinal axis.
The second stage of the laboratory study included an assessment of the resistance to stress of non-vital teeth with varying degrees of destruction of the coronal part. The study was carried out in vitro
on 160 premolars and molars removed for periodontal and orthodontic reasons in patients aged 21 to 63 years. The teeth used in the study met the following criteria: (1) belonging to the groups of premolars and molars; (2) the presence of 4 walls in an intact state, not counting the occlusal surface; (3) no previous endodontic treatment; (4) presence of one root and one root canal; (5) the preserved walls were located above the level of the enamel-cementum junction; (6) the thickness of the preserved walls is at least 1 mm; (7) absence of apical resorption or root caries; (8) no root fractures or cracks.
To assess the degree of destruction of the coronal part of the teeth, the index of destruction of the occlusal surface of the teeth (IDOSI) was used. Defects in the coronal part of the studied teeth were assessed according to the classification proposed by I. Peroz et al. in 2005. The correspondence between the Peroz and IROPZ classifications is described in Table. 2. In our study, we used teeth whose destruction corresponded to Peroz classes II, III and IV.
Table 2. Description of defects in the coronal part of the tooth using the Peroz classification and the IROPD index
All studied tooth samples were divided into six groups, 23 teeth in each, depending on the number of preserved coronal walls, as well as the characteristics of direct tooth restoration.
Group 1 included teeth of class II according to Peroz (IROPD 0.5–0.6) with three preserved walls, restored with a dual-curing nanocomposite LuxaCore Z-Dual ( n
=23), 2nd group - teeth of class III according to Peroz (IROPD 0.6-0.7) with two preserved walls, restored with LuxaCore Z-Dual nanocomposite (
n
=23);
Group 3 - teeth of class IV according to Peroz (IROPS 0.7-0.8) with one preserved wall, restored with LuxaCore Z-Dual nanocomposite ( n
= 23).
Group A included teeth of class II according to Peroz (IROPS 0.5–0.6) with three preserved walls, restored with LuxaCore Z-Dual nanocomposite and glass fiber reinforced composite with LuxaPost pin ( n
=23);
group B - teeth of class III according to Peroz (IROPS 0.6-0.7) with two preserved walls, restored with LuxaCore Z-Dual nanocomposite and glass fiber reinforced composite with LuxaPost pin ( n
= 23);
group C - teeth of class IV according to Peroz (IROPS 0.7-0.8) with one preserved wall, restored with LuxaCore Z-Dual nanocomposite and glass fiber reinforced composite with LuxaPost pin ( n
= 23).
Intact teeth served as a control group ( n
=23), mechanically cleaned from fragments of soft tissue and dental plaque.
When preparing dental samples for laboratory research, we completely reproduced the sequence of mechanical and chemical treatment during endodontic treatment of teeth with coronal defects, used in clinical practice. Further tactics for restoring the coronal part of the experimental samples depended on which group the tooth under study belonged to. At the same time, all the steps performed for direct restoration of the coronal part of teeth in clinical practice were observed.
The second stage was a clinical study, in which the results of treatment of 109 patients aged 20 to 63 years were analyzed, including 42 men and 67 women, who underwent restoration of 146 premolars and molars with varying degrees of coronal destruction.
Mechanical treatment of the root canals was performed using ProTaper nickel-titanium instruments. Medicinal treatment was carried out in accordance with generally accepted methods; endodontic treatment was performed under the control of an iPex apex locator (NSK) and x-ray control. In the presence of periapical inflammation, temporary filling was performed.
AN Plus sealer (Dentsply) was used as an endosealant. The root canal orifice was isolated with light-curing glass ionomer lining cement Vitrebond (3M ESPE) and a temporary filling was placed with Fuji IX GP glass ionomer cement (FAST) (GC Corporation). Further treatment was continued after 48-72 hours.
The main group included 75 teeth, including 34 premolars and 41 molars, which were restored in 56 people (36 women and 20 men aged 20 to 63 years) using LuxaCore Z-Dual dual-curing nanocomposite material supported by glass fiber reinforced composite LuxaPost pins, maintaining at least 4 mm of gutta-percha in the apical third of the root canal.
Within the group, the teeth were distributed depending on the type of defect in accordance with the Peroz classification and the IROPD index:
— three intact walls of the coronal part (class II according to Peroz, IROPZ 0.5–0.6) — 24 teeth (32.0%);
- two intact walls of the coronal part (III class according to Peroz, IROPZ 0.6-0.7) - 26 teeth (34.7%);
- one intact side wall (IV class according to Peroz, IROPZ 0.7-0.8) - 25 teeth (33.3%).
The comparison group included 71 teeth, 34 premolars and 37 molars, which were restored in 53 patients (31 women and 22 men aged 20 to 61 years) using LuxaCore Z-Dual dual-curing nanocomposite material, removing gutta-percha from the orifice root canal by 2-2.5 mm. The distribution of teeth into subgroups according to the number of intact walls of the coronal part was as follows:
— three preserved walls (class II according to Peroz, IROPZ 0.5–0.6) — 23 teeth (32.4%);
- two intact walls (III class according to Peroz, IROPZ 0.6-0.7) - 25 teeth (35.2%);
- one intact wall (IV class according to Peroz, IROPZ 0.7-0.8) - 23 teeth, which corresponded to 32.4%.
In total, during the study, we restored 68 premolars and 78 molars with coronal defects corresponding to Peroz classes II (32.2%), III (34.9%) and IV (32.9%).
Assessment of the quality of the restoration was also carried out in all patients immediately after treatment and after 6, 12, 18 and 24 months based on a comprehensive clinical and radiological examination, including examination and probing, in accordance with the Ryge criteria. In patients of the main group, the quality of fixation of a fiberglass composite-reinforced pin was determined. Treatment results were characterized as “good”, “satisfactory” and “unsatisfactory”. We carried out an electrometric assessment of the quality of marginal adaptation of fillings if the criterion for their marginal fit according to Ryge met the “A” score. The quality of the marginal seal was considered satisfactory when readings from the DENTEST device ranged from 0.1 to 2 μA.
For statistical processing and comparison of the results obtained during the laboratory study, the Student's test was used. The significance of changes in the parameters of restored teeth detected during clinical assessment of the quality of restorations was calculated using the Friedman test.
Pin installation
The pin is installed in the root canal of the tooth, filled with gutta-percha, at the end of endodontic treatment. To do this, part of the gutta-percha is removed, a pin is inserted into the canal and fixed with cement. The top of the tooth is covered with filling material in order to restore its anatomical shape. If necessary, an artificial crown is placed on the tooth.
Installation of root pins and pin inlays is an important stage in tooth restoration using fixed dentures.
If the crown part of a tooth is completely destroyed, it is restored using standard pins, cast core inlays, standard pins made of carbon fibers, and other structures.
Methods of dental restoration after endodontic treatment
Severely damaged teeth must be strengthened with additional means. This will help avoid fracture of the tooth stump and maintain its strength for a long time. Intra-canal pins and stump inlays are used as support. The choice of support element depends on how badly the tooth is damaged and what method will be used to restore it. Installation of an intracanal pin is advisable if there are only two walls of the crown, the height of which should not be less than three millimeters.
Polymer tab
With a polymer inlay, these stress and deformation indicators are as close as possible and, as a result, the percentage of vertical tooth root fractures when using fiber pins is virtually reduced to zero.
But there is another problem here. When producing metal cast core inlays, we achieved precise adaptation to the lumen of the root canal. When fixing the fiber post using the adhesive technique, we compensated for this discrepancy with composite cement.
It would seem that everything is fine, BUT the root canal has one of the highest C-factor indicators (the ratio of bonded to free surfaces). The higher this indicator, the higher the stress at the ligament boundary. And the shorter the service life of the adhesive bond.
There is a solution - making an individual
Dental reconstruction
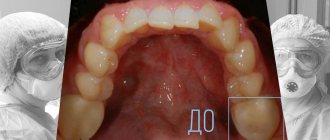
The property of composites to firmly bind to the hard tissues of teeth has made it possible to use these materials to correct the shape, color, minor anomalies in the position of teeth in the dentition, and solve purely aesthetic problems. Such a change in the shape, color, and transparency of the crowns of natural teeth is called dental reconstruction. It’s long and difficult to talk about the technique of carrying out such work, but is it necessary? Let me use some examples to clearly show how teeth can be reconstructed and their aesthetics improved.
Closure of diastemas and trema
Diastemas (a gap between the central teeth) and trema (a gap between the teeth) cause a lot of grief to people who have such (in their opinion) defect; they may even develop an inferiority complex. Although some people do not consider this a defect, but, on the contrary, a kind of highlight.
Patient K. after orthodontic treatment. The dentition was restored, the three teeth disturbed the aesthetics. On 2 visits, the teeth were closed by reconstructing the central and lateral incisors (see photo above). The young girl wanted to change the shape and color of the fangs, which was done on the third visit (see photo below)
Restoration of traumatic fractures of dental crowns
Often, teeth suffer as a result of injuries when a minor chip or fracture of the tooth crown occurs. Usually there is a tooth bruise. Patients complain of minor or intense pain. It is necessary to exclude traumatic inflammation of the nerve, to ensure that reversible or irreversible phenomena have occurred in the dental pulp. If necessary, the nerve is removed and endodontic treatment of the tooth is performed. As the pain gradually subsides, the patient is under medical supervision. If after 7-10 days the pain does not bother you, you can restore the tooth crown.
After anesthesia, gentle preparation of the hard tissues of the tooth is carried out. A small layer of hard tissue is removed on the surface of the chipped tooth crown in the form of bevels. This is necessary to increase the area of contact of the material with the tooth surface, as well as for a smooth transition of the composite to the tooth. Subsequently, it is necessary to take control x-rays of the injured teeth to exclude complications in the long-term period after the injury.