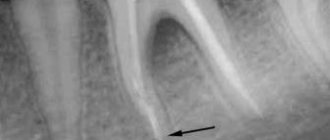
Local anesthesia is used to numb sensations in a specific part of the body. This prevents pain during surgical procedures.
An anesthetic is applied to the part of the body that is undergoing surgery.
Can be used for sedation, which calms the patient and reduces stress levels. Together, they allow the surgeon to perform the procedure without pain or distress.
Local anesthesia does not last long, so it is mainly used for small outpatient procedures where the patient can leave the clinic the same day.
Benefit
Local anesthesia provides pain relief for dental surgery and other outpatient procedures.
Local anesthesia is used when:
- the operation is minor and does not require general or regional anesthesia
- the procedure can be performed quickly and the patient does not have to stay overnight
- the operation does not require muscle relaxation or loss of consciousness of the patient
Examples include dental surgery, removal of warts, moles or cataracts, and biopsy.
Choice of local anesthetic
articaine anesthetics are recommended and widely used (Zoryan E.V., Rabinovich S.A., Matveeva E.G., 2007; Rabinovich S.A., Vasiliev Yu.L. , 2011). This is due to a number of pharmacological properties. Articaine 4% has relatively low fat solubility compared to lidocaine and mepivacaine and passes less through histohematic barriers.
The metabolism of articaine occurs much faster compared to other anesthetics. Thus, the half-life (t1/2) of articaine is 20 minutes, t1/2 of lidocaine is 90 minutes, t1/2 of mepivacaine is 114 minutes.
Other amide anesthetics: mepivacaine, lidocaine - are the anesthetics of choice in pediatric dentistry for a number of reasons. In the Russian Federation, 2% lidocaine is not available in carpuled form and its use in pediatric practice is limited by the capabilities of outdated technology: ampoules, plastic syringes, large-sized and diameter needles.
Mepivacaine 3% does not contain preservatives or vasoconstrictors. This anesthetic is recommended for use if a child has a concomitant pathology and is intended for short-term interventions. In children with bronchial asthma, the use of 3% mepivacaine (without epinephrine) for local anesthesia is indicated (Zoryan E.V., Rabinovich S.A., Matveeva E.G., 2008). This is due to the fact that this drug does not contain sulfites (epinephrine stabilizer), which can cause an attack of bronchospasm.
Children with pathologies of the cardiovascular system, including congenital ones in the compensation stage, are at risk of developing complications. The use of vasoconstrictors in this category of patients is relatively contraindicated. If possible, non-vasoconstrictor anesthetics should be used, such as 3% mepivacaine.
Types of Local Anesthesia
The type and dose of anesthesia will depend on many factors. These include patients' age, weight, allergies, body part being operated on, and any current health conditions.
Various drugs are used to block pain. They can be applied by injection or by applying a spray or ointment.
The drug works by targeting specific nerve pathways to prevent the nerves in the area of application from sending signals to the brain.
Typically, the drug takes effect within a few minutes and wears off within a few hours. A stronger and higher dose will last longer.
Cocaine was the first anesthetic, but is now rarely used. Lidocaine is currently the most widely used local anesthetic, but different drugs are used for different purposes.
For longer procedures, bupivacaine is more suitable, but it may be more painful when first used. Therefore, the anesthesiologist may use lidocaine first and then administer bupivacaine if numbness is required for a longer period.
Synthetic anesthetics are similar in structure to cocaine, but these drugs do not have the same potential for abuse.
Drugs used
The success of conduction anesthesia depends not only on the technique used, but also on the drugs used. The following medications are used for this pain relief technique:
- Solutions of the Articaine series. They have a long lifespan and high efficiency. These include:
- Ultracaine.
- Septanest.
- Ubistezin.
- Lidocaine. It is a highly effective anesthetic and at the same time contains a minimal amount of toxic substances.
- Melivacaine. The duration of action of this drug is about 40 minutes. Melivacaine has no contraindications for use.
- Novocaine. This is perhaps the most frequently used remedy. It is characterized by low toxicity and rapid hydrolysis in the body.
Preparing for local anesthesia
If the patient is undergoing surgery with local anesthesia, the doctor should explain in advance how to prepare.
Patients should tell their doctor if they are using any medications, especially if they are blood thinning agents such as aspirin or warfarin.
Your doctor may instruct you not to eat anything for several hours before surgery. It is also important not to drink alcohol for 24 hours before taking the anesthetic.
In the doctor's office, the doctor applies a local anesthetic to the appropriate area of the body. It will start to feel numb.
The doctor will not act if the patient does not feel numb.
The anesthetic will prevent any pain, but the patient may still feel pressure during surgery.
Depending on what the procedure is and how anxious the patient feels, a sedative may be prescribed at the same time. This will help the patient feel calm and less anxious.
The doctor will monitor the amount of oxygen in your blood using a small device placed on your finger. In rare cases, a plastic nasal tube will be used to provide supplemental oxygen.
Advantages and disadvantages of conduction anesthesia
Advantages:
- The drug can be administered outside the surgical site.
- Anesthesia has a long-lasting effect. A specialist can monitor the duration of action of the medication.
- To achieve the desired effect, small doses of painkillers are sufficient.
- There is no deformation of soft tissues in the operated area.
- When exposed to conduction anesthesia, salivary activity decreases.
- The technique is safe, so it can be used from the age of 12, and also in some cases in pregnant and lactating women.
- The cost of the procedure is affordable.
Flaws:
- In order for anesthesia to pass without complications, the specialist must have certain skills and sufficient experience.
- There is a high probability of the anesthetic entering a blood vessel.
- Restricted use by age (only from 12 years old).
- Risk of injury to nerves or blood vessels.
Risks and complications
Local anesthesia is generally considered very safe. For minor surgeries it is safer than general anesthesia.
There may be tingling and pain, and there may be bruising as you take the drug and wear it off, but this is usually minor.
A person who has had local anesthesia must be careful not to get hurt when they cannot feel pain, such as when biting their cheek after dental treatment.
Temporary side effects that affect some people include:
- blurred vision, dizziness and vomiting
- headache
- muscle twitching
- persistent numbness, weakness, or tingling
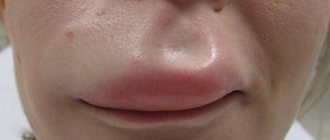
Some people may have an allergic reaction. The patient may experience hives, itching, and difficulty breathing.
Cyanosis may occur, in which the skin turns bluish due to poor circulation or insufficient oxygenation of the blood.
In very severe cases, a person may experience CNS depression, in which the central nervous system slows down too much, resulting in a decrease in breathing and heart rate. This can lead to cardiac arrest if blood stops pumping to the heart.
An overdose of local anesthetic can lead to seizures. This can be life-threatening.
It is impossible to imagine modern dentistry without local anesthesia. Most therapeutic, some orthopedic and almost all surgical interventions are performed after preliminary anesthesia. Articaine-containing local anesthetics, widely used and deservedly considered the most effective and safe, allow many complications to be avoided if the rules of their use are followed correctly [3]. But they also use lidocaine and even procaine (Novocaine), and in maxillofacial surgery - ropivacaine for long-term intra- and postoperative pain relief, so doctors should be well aware of how great the risk of complications is directly associated with the use of local anesthetics (see diagram) .
Let us dwell on systemic toxic reactions to local anesthetics - one of the little-studied complications that can lead to a critical outcome. In contrast to allergic reactions, systemic toxic reactions to local anesthetics are common, especially when high doses of drugs are used. Over the past decades, scientists around the world have carried out a great deal of research and analytical work to study the toxic effect of local anesthetics on the human body and determine the leading signs that distinguish this complication from allergic reactions. The published results of statistical studies convincingly indicate that modern local anesthetic drugs are much less dangerous as allergens (the risk of allergy is 1:2,000,000 injections) and much more likely to cause systemic toxic reactions (the risk is estimated as 1:1000 injections) [12].
Systemic toxic reactions to local anesthetics in maxillofacial surgery and dental practice, in contrast to general surgery, where these drugs are administered in much larger quantities for the purpose of regional anesthesia, are less common, but this complication must be remembered due to the likelihood of a tragic outcome. .
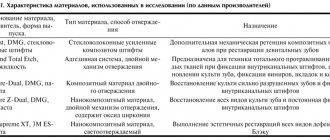
The modern market provides dentists with a wide selection of local anesthetics. When determining the safest drug, it is important to focus primarily on its anesthetic index, duration of effective action and compatibility with other drugs taken by the patient. In table 1 provides information on the maximum doses, duration of action, activity and toxicity of local anesthetics.
Table 1. Anesthetic activity, duration of action, toxicity and maximum permissible dose of various local anesthetics Note. m/a - local anesthetic; m/a+iv/c - local anesthetic with vasoconstrictor; activity - the ratio of the minimum effective dose of novocaine to the minimum effective dose of another drug; toxicity - the ratio of the minimum lethal dose of novocaine to the minimum lethal dose of another drug; anesthetic index is the ratio of the potency of the drug to the relative toxicity of the drug.
The analgesic effect of a local anesthetic is determined by its vasoactivity, lipid solubility, ability to bind to proteins and acidity. Certain adjustments, of course, are made by the somatic status of the patients, as well as the pharmacological interactions that occur in the case of basic drug therapy.
The rate of onset of the analgesic effect, systemic absorption, metabolism and elimination of the local anesthetic determine its physicochemical properties. Thus, the lipid solubility and protein-binding characteristics of a local anesthetic depend on its affinity for the cell membrane of the neuron, which consists of fat (90%) and protein (10%). The higher the fat solubility of the drug, the easier it penetrates the membrane, and therefore the more effective. The better the anesthetic binds to protein, the longer its duration of action. The dissociation constant of the drug determines the rate of onset of the analgesic effect, as well as absorption and elimination.
After injection, part of the anesthetic diffuses onto the neuron membrane; the remaining drug enters the vascular bed. Increased absorption of local anesthetic equates to direct entry into the vessel; This should be especially feared in the acidic environment of the inflammatory focus. The amount of drug absorbed by the vessels depends on vascularization and the amount of blood flow in the anesthetized tissue, as well as the effect of the local anesthetic on the tone of the vascular wall. During infiltration anesthesia, amide anesthetics of medium and long action cause vasodilation, and ropivacaine (naropin), unlike other long-acting drugs (bupivacaine hydrochloride - marcaine), gives a vasoconstrictor effect. If a local anesthetic drug contains a vasoconstrictor, the rate of systemic absorption slows down, but there is a risk of developing tachycardia and atrial fibrillation.
Until recently, it was believed that the degree of systemic toxicity was strictly dependent on the concentration and amount of anesthetic administered. Thus, using lidocaine as an example (Fig. 1), peak levels of anesthetic concentrations in blood plasma were shown, which determine the possible clinical picture of a systemic toxic reaction.
Rice. 1. Dependence of the clinical manifestations of the systemic toxic reaction of lidocaine on the level of its plasma concentration.
However, according to recent publications, the described cases of systemic toxicity of local anesthetics in the practice of general and maxillofacial surgery have suggested that the manifestation of toxic reactions does not always depend on the excessive amount of administered anesthetic; even the doses of drugs recommended for use can cause this complication [6, 16, 18].
Clinically, the systemic toxic effect of local anesthetics is more often manifested by symptoms of central nervous system damage and less often by cardiovascular damage. Due to the variety of conditions that determine the timing and rate of entry of the local anesthetic drug into the vascular bed, the period of development of clinical symptoms of systemic toxicity varies within a fairly wide range - from 1-5 to >60 minutes [10].
Based on the severity of clinical symptoms, systemic toxicity of local anesthetics is divided into 3 degrees [2]. If its degree is mild (minor toxic reactions), the patient’s first complaints are tingling and itching in the area where the anesthetic was administered; these sensations may spread to the lips and tongue. At the same time, tinnitus and a metallic taste in the mouth appear. Breathing and hemodynamics are not impaired, moderate tachycardia may be observed. Since the patient's consciousness is preserved, changes in well-being, as a rule, do not go unnoticed; they cause the patient a certain anxiety, which increases as the symptoms intensify; a feeling of fear is often added. The clinical picture of the development of a toxic reaction may be limited to this; gradually the unpleasant sensations disappear without additional therapeutic measures, and the patient calms down. Most often, mild complications of local anesthesia go unnoticed by the doctor and are not recorded in the medical history. But if the patient’s subjective sensations are accompanied by trembling, twitching of individual muscles, nausea, possibly vomiting, and signs of impaired consciousness, in particular orientation, are noted, it should be understood that the toxic reaction develops and becomes moderately severe. With the maximum severity of clinical manifestations at this stage, the patient’s consciousness becomes confused, speech is impaired, numbness and retardation are characteristic, rapid breathing, decreased blood pressure, bradycardia, motor agitation or convulsions are noted. The appearance of seizures indicates that the systemic toxic reaction is becoming severe. Against the background of convulsions, loss of consciousness, decreased muscle tone, respiratory failure up to apnea, arrhythmias, asystole, relaxation and paralysis of the sphincters can occur. Without providing emergency care to patients in critical condition, including resuscitation measures with mandatory specific elements, death is inevitable.
A systemic toxic reaction to local anesthetics is not necessarily clinically manifested by all of the listed signs; some of them are often observed. An analysis of 93 cases of systemic toxicity of local anesthetics showed that the classic clinical picture developed in only 60% of victims; the predominance of pathological signs of the central nervous system with cardiovascular disorders is observed in 30.3% of cases, and only isolated cardiovascular disorders are described in 9.7% of patients [10].
The frequency of clinical signs indicating the development of a systemic toxic reaction following accidental intravascular administration of a local anesthetic is presented in Fig. 2.
Rice. 2. Frequency of development of clinical signs of toxic effects of local anesthetics [7].
Due to the complexity of conducting studies (it is impossible to perform them on humans!), the mechanism of development of systemic toxicity remains unclear. Today it is known that local anesthetics inhibit the process of oxidative phosphorylation, so the most severe disorders occur in the organs that are least adapted to anaerobic respiration metabolism, and this is primarily the brain and heart [2].
It is believed that the toxic effect on brain cells determines the ability of a local anesthetic to penetrate the blood-brain barrier and block sodium channels of excitable cell membranes, which causes toxic reactions of varying severity. If a convulsive syndrome occurs, the accompanying metabolic acidosis increases the uptake of the drug not only by brain neurons, but also by cardiomyocytes.
Cardiotoxicity is probably primarily determined by the ability of local anesthetics to reversibly bind to the intracellular part of the voltage-gated sodium channels of the cardiomyocyte, preventing them from opening and thereby preventing the generation of an action potential and its propagation along the nerve fiber. And the higher this ability of the anesthetic, the stronger its analgesic effect, but at the same time, the inhibitory effect on the conduction system of the heart [8].
All local anesthetics in high concentrations increase the refractory period of the heart, inhibit the excitability, contractility and conductivity of the myocardium - which means that in doses exceeding permissible concentrations, any of the local anesthetic drugs can cause severe depression of the myocardium. It is important to note that the clinical picture of systemic toxicity caused by lidocaine is manifested primarily by severe pathological reactions from the central nervous system; this allows the doctor to take the necessary measures to save the patient in time. And drugs that are more powerful than lidocaine, even in what is considered an acceptable plasma concentration, can, without causing convulsive manifestations or reducing myocardial contractility, provoke arrhythmias of varying severity [8].
Particular care when performing local anesthesia is required in patients with risk factors for systemic toxicity; these include anemia; hypoproteinemia; chronic heart failure with congestion; impaired liver and kidney function; endocrine and metabolic diseases; pregnancy; old age and young age (children). Compared with adults, young children have a significantly higher ratio of cardiac output and regional blood flow to body weight, and systemic toxic reactions develop more quickly in children due to the rapid increase in peak toxic drug concentrations in plasma. Thus, in a 3-year-old child after topical anesthesia, almost instantaneous absorption of the local anesthetic occurs, and the time for the onset of peak plasma concentration of lidocaine during infiltration anesthesia is comparable to that during its intravenous administration.
Special attention should be paid to the treatment of patients under sedation and general anesthesia using local anesthetics. The literature [10] describes 2 cases of systemic toxicity in infants 6 and 9 months old during uranoplasty under general anesthesia a few minutes after infiltration of local anesthetic (in one case, lidocaine, in the other, articaine). The emerging convulsive syndrome left no doubt about the diagnosis, and assistance was provided in a timely manner. Upon completion of postoperative rehabilitation, patients were discharged from the hospital without neurological deficit. Analysis of other episodes of systemic toxicity occurring during general anesthesia shows that signs of cardiovascular complications are more common because the central nervous system is blocked and early symptoms go unnoticed.
Prevention of toxic effects of local anesthetics
A systemic toxic reaction can be anticipated in cases of planned treatment of patients at risk, when the recommended dose of anesthetics is exceeded, or in non-compliance with anesthesia techniques. But, unfortunately, there is no guaranteed option to prevent this complication [15].
Prevention of systemic toxicity consists of strict adherence to instructions for the use of local anesthetics, correct execution of anesthesia techniques and careful attention to the patient both at the stage of preparation for treatment and during it.
During the initial consultation, be sure to find out complete information about the patient’s health. If you have concomitant somatic diseases, obtain an extract from the medical history indicating the diagnosis and the basic therapy recommended for use. If necessary, conduct additional examination. Before treatment, be sure to determine the patient’s physical condition and record the main parameters (blood pressure, heart rate, respiratory rate) in the medical history. Be sure to inform the patient about the possible risks and obtain his written consent for all planned interventions [3].
When choosing a local anesthetic drug, be sure to choose the least toxic of them, if the situation allows it. The use of long-acting local anesthetics is justified for long-term interventions that require prolonged postoperative pain relief, and only if a full set of resuscitation equipment is available.
Be sure to use the minimum effective dose of local anesthetic, choose a sufficient concentration and do not exceed the required volume of anesthetic. Consider the absorption capacity of the surrounding tissues at the injection site [4].
Before administering the anesthetic, be sure to perform an aspiration test and repeat it if you move the needle along the injection; Do not forget that the results of the aspiration test are false negative in approximately 2% of cases. To increase safety, use ultrasound guidance during injection whenever possible, although its effectiveness has not yet been studied and the risk of intravascular injection of anesthetic remains [5].
Be sure to inject the local anesthetic gradually, slowly (1 ml/min) or fractionally with pauses of 15-30 s. When introducing large portions of anesthetic, the injection interval must be increased to reduce accumulation [4].
Do not interrupt verbal contact with the patient during local anesthesia; be sure to monitor his reaction during manipulation and actively identify complaints - this increases the likelihood that the first subjective signs of a developing systemic toxic reaction will be noticed by you on time [3].
Below are the maximum permissible doses of local anesthetics most used in outpatient dental practice for children and adults (Tables 2-5).
Table 2. Maximum permissible doses of lidocaine 2%
Table 3. Maximum permissible doses of mepivacaine 2%
Table 4. Maximum permissible doses of articaine 4%
Table 5. Maximum permissible doses of mepivacaine 3%
Therapeutic measures for systemic toxic reactions
Until recently, the treatment of systemic toxic disorders caused by local anesthetics included the use of anticonvulsants, ensuring adequate oxygenation of the patient up to tracheal intubation followed by artificial ventilation, infusion therapy with large volumes of blood substitutes with the introduction of glucocorticosteroids and drugs that correct cardiovascular disorders. Carrying out cardiopulmonary-cerebral resuscitation, if necessary, did not include any special features; the complex was performed according to the general protocol [1].
Currently, along with measures to replace the patient’s vital functions, the priority in the treatment of systemic toxicity is to reduce and, if possible, eliminate the systemic effect of local anesthetics [13]. The recommended intravenous administration of lipid solutions, the effectiveness of which has been proven experimentally and clinically [9], allows the symptoms of toxicity to be relieved by binding lipophilic local anesthetics. The plasma concentration of drugs decreases, they are “washed out” (detached along the concentration gradient from the membrane of the neuron and cardiomyocyte) and removed with new portions of lipid. In addition, it is known that lipid-containing solutions are an energy substrate for cardiac mitochondria and this ability is in demand in the case of cardiotoxic reactions. The treatment regimen using Intralipid solution (20%) to eliminate systemic toxic reactions of local anesthetics was called “lipid rescue” [7].
The clinical picture of the severe stage of systemic toxicity of local anesthetics can develop rapidly, so it is very important to correctly assess the first symptoms and begin emergency care in a timely manner. Seizure syndrome remains an absolute indication for the use of benzodiazepines; it is more dangerous to treat it with propofol or ultra-short-acting barbiturates due to their own pronounced cardiodepressive effect. As in previous recommendations, one of the first measures to save the patient is to ensure adequate oxygenation by any available means, including tracheal intubation and mechanical ventilation with 100% oxygen. In case of ineffective blood circulation due to arrhythmia or asystole, resuscitation measures should be started immediately and continued for at least 60 minutes. Since local anesthetics do not cause irreversible changes in the myocardium, with sufficient oxygenation of the brain and the administration of lipid solutions during this time, there is hope for saving the patient. It is extremely important not to rush to stop effective resuscitation measures if systemic toxicity is caused by powerful anesthetics, because they take a long time to “wash out” [6]. When carrying out symptomatic therapy, if necessary, it is necessary to avoid the administration of lipophilic drugs - beta-blockers and calcium channel blockers, abandon vasopressin, use only amiodarone (cordarone) to relieve ventricular arrhythmias, reduce the dosage of epinephrine (adrenaline) to less than 0.1 mcg/day. kg or completely abandon its administration [13].
Literature sources [20] report that in case of a systemic toxic reaction to local anesthetics, rapid administration of large volumes of lipid solutions is not accompanied by significant complications, and their clinical effectiveness against the background of resuscitation measures allows one to avoid residual cardiac disorders and neurological deficits [10, 17].
For “lipid leaching,” any fat emulsion can be used, but Intralipid (20%) has proven itself to be the best [11]. Inactivation of local anesthetics with diprivan (propofol) should not be carried out due to the need for a large amount of the drug to obtain a positive result due to its low lipid content, and this is dangerous since diprivan has a direct cardiodepressive effect [15]. Today, it is recommended to relieve a systemic toxic reaction to local anesthetics with lipids, starting the administration of the drug when the first characteristic complaints or symptoms appear and at the same time being ready to perform a full range of resuscitation measures [6].
In each medical institution, including dental, where local anesthetics are used, it is necessary to have 1 liter of fat emulsion solution (Intralipid 20% - 500 ml or other), syringes for “lipid washing out” with a volume of 50 ml, peripheral intravenous catheters 14-16 G, Infusion systems, copy of the Lipid Rescue protocol [19].
After catheterization of the peripheral vein, the lipid solution must be administered as a bolus (Intralipid 20% - 1.5 ml/kg) using 50 ml syringes, then switch to drip infusion (Intralipid 20%, rate - 0.25 ml/kg/min) and Continue administering the drug at this pace for at least 10 minutes after blood circulation has stabilized. If it is not possible to stabilize blood circulation with this dose of lipid solution, it is necessary to repeat its bolus administration in the same dosage (Intralipid 20% - 1.5 ml/kg) and switch to an accelerated infusion of the drug (Intralipid 20%, rate - 0.5 ml/kg /min). The highest single dose of fat emulsion is acceptable - 10 ml/kg/min.
At the Euroanaesthesia 2010 forum in Helsinki (Finland), the European Board of Anesthesiology, together with the European Society of Anaesthesiology, adopted a declaration on patient safety in anesthesiology. It provides fundamental points that make it possible to prevent and avoid serious complications and prevent danger to patients. In particular, it is stated that all medical institutions that use local anesthetics “... must have protocols and facilities necessary in situations of systemic toxicity...” [14]. The Declaration of Helsinki has been endorsed by the World Health Organization, the World Federation of Societies of Anaesthesiologists and the European Patients Federation. Taking into account its specifics, each country has the right to refine and adapt the protocol for resuscitation using lipid solutions to its own conditions. We consider this task extremely important for our medical community.
The authors declare no conflict of interest.
Other applications
Local anesthesia may also be used to diagnose some chronic conditions and to relieve pain after surgery.
Research has shown that local anesthesia may be more useful than opioids such as morphine for treating pain after total knee replacement surgery.
In 2010, results from a rodent study in Turkey showed that local anesthetics may reduce some symptoms of inflammatory bowel disease (IBD).
Anyone administering any type of anesthetic should be appropriately trained and qualified.
FEATURES OF PAIN RELIEF OF TEMPORARY TEETH
Of course, the choice of pain relief method depends on the planned intervention.
In the treatment of caries and pulpitis of temporary teeth, preference is given to infiltration methods carried out from the vestibular (buccal/labial) side, and there is no need for lingual or palatal anesthesia. This is explained by the predominance of spongy substance and a large number of nutrient openings in the structure of the jaw bones, facilitating the diffusion of local anesthetic.
In order to reduce the degree of pain of the injection and increase the level of comfort for the child, the following recommendations for local anesthesia should be followed:
- A preliminary distracting preparatory conversation with the child is necessary, during which the doctor uses terms that the child understands. In this case, the words “injection”, “syringe”, “anesthesia”, “removal”, “needle” are not pronounced.
- The child should not see (look at) the injection equipment. All instruments are presented by an assistant out of sight of the child.
- Application anesthesia should be performed so that the child does not feel the puncture stage of the mucous membrane.
- The rule must be observed: “one needle, one injection.” If the needle accidentally comes into contact with the bone tissue of the jaw, its tip is deformed; as a rule, it bends in the direction opposite to the bevel. A repeated injection with the same “dull” needle in another segment will involve applying pressure that is unpleasant for the child.
- The anesthetic should be injected slowly, 1 ml/min. Forced administration of the anesthetic leads to hydrodynamic tissue trauma, which causes pain.
- Two-stage injection of a portion of anesthetic. When performing infiltration anesthesia, the doctor initially injects a small amount of anesthetic? 0.1 submucosally, while a zone of tissue infiltration the size of a millet grain is visually determined. Next, the doctor talks with the child for 2-3 minutes.
- The subsequent administration of the main portion of the anesthetic is painless.
- The temperature of the anesthetic solution should be close to the child’s body temperature. To do this, do not store anesthetic carpules in the refrigerator. Before the injection, the doctor can “warm” the carpule in his hand or in running hot water.
The volume of injected anesthetic for infiltration anesthesia of temporary incisors and canines is on average 0.3 ml; for anesthesia of temporary molars, 0.5-0.6 ml is used. Subperiosteal anesthesia should not be performed as this will cause pain to the child and will not increase effectiveness. The needle should move submucosally towards the apexes of the roots of the teeth. In the upper jaw, when performing infiltration anesthesia, one should not insert a needle into the area of the frenulum of the upper lip, mucous strands in the area of temporary canines. These areas have an extensive network of nerves, providing hypersensitivity in these areas.
When performing an operation to remove temporary teeth of the upper jaw with a diagnosis of periodontitis, various combinations of infiltration methods are used. In the upper jaw, when removing incisors and canines, infiltration vestibular (0.5 ml) and incisal anesthesia (less than 0.2 ml) is used. In this case, classical conduction anesthesia with the advancement of the needle into the incisive canal is not carried out, but a certain amount of anesthetic is injected on the side of the incisive papilla, until signs of ischemia appear. If possible, painful incisal anesthesia should be avoided, which can be replaced with topical anesthesia or by inserting a needle into the vestibular interdental papilla and then moving it to the palatal side with a continuous supply of anesthetic.
When anesthetizing the first and second temporary molars, infiltration vestibular (0.5-0.6 ml) and palatal (0.2 ml) anesthesia is used. Palatal anesthesia can be replaced by the above-described approach through the interdental papilla. To reduce the degree of pain of local anesthetic injection into the hard palate, preliminary application anesthesia should be used.
When removing temporary teeth of the lower jaw with a diagnosis of periodontitis, a combination of conduction and infiltration methods is used. When removing incisors and canines, infiltration vestibular (0.3 ml) and lingual (less than 0.2 ml) anesthesia is used. Lingual infiltration anesthesia is performed in the area of the transition of the attached gum to the mobile mucosa of the floor of the mouth. The anesthetic is injected into the submucosal layer; the needle is not advanced to prevent intravascular injection.
You can anesthetize the lingual mucosa by inserting a needle into the interdental papilla from the vestibular side and then moving it towards the lingual mucosa. When removing temporary first molars of the lower jaw, the above-described technique is used with the only difference that 0.5 ml of anesthetic is injected from the vestibular side of the tooth being removed. In the presence of local inflammation, it is necessary to perform conduction mental anesthesia. When removing the second temporary molars of the lower jaw with a diagnosis of periodontitis, either mandibular anesthesia (1 ml) or a combination of mental anesthesia (0.6 ml) and lingual infiltration (0.2 ml) is performed.
During the period of physiological change in occlusion, the removal of temporary teeth for orthodontic indications has some features. The most common mistake is removing a “moving” tooth under application anesthesia. The depth of application anesthesia is 2-3 mm of the mucous membrane, and the roots of the tooth may not be completely resorbed, and their removal will be painful. Application anesthesia can be used as an independent method only if the tooth is fixed by mucous membrane on one edge. In other cases, infiltration anesthesia should be performed. The anesthetic is administered before signs of gum ischemia appear; its volume is minimal.
Alveolar pain (alveolar pain)
Most patients experience alveolar pain in the area of the extracted tooth after the anesthesia wears off. Its intensity is moderate and it gradually disappears. In other patients, after the anesthesia wears off, pain occurs when the tongue touches the gum in the area of the extracted tooth, while eating, or while brushing teeth. Along with this, a number of patients suffer from constant intense pain that does not stop for several days, debilitating the patient. The mechanism of occurrence of these pains is different.
- The appearance of pain after the cessation of the anesthetic is a natural reaction to tissue injury: biologically active substances are released, which are specific irritants for pain receptors.
- The occurrence of aseptic inflammation in the wound. It is a necessary link in the process of reparative regeneration and is also accompanied by the release of biologically active substances. Pain of moderate intensity appears within 1-2 days after tooth extraction.
- The pain that occurs when the tongue touches the surgical area while eating, talking, or brushing teeth is caused by mechanical irritation of pain receptors (often by the sharp edge of the alveoli).
- Constant intense pain, debilitating the patient, is characteristic of a purulent-inflammatory process with a pronounced necrotic component.
- Pain caused by the presence of sharp edges of the socket, movable fragments of the edge of the socket that have retained their connection with the gum.
Clinical picture of alveolar pain
Complaints of pain that occurs while eating, talking, brushing teeth, touching the tongue to the gum in the area of the extracted tooth. Upon examination, the edges of the gums in the area of the socket of the extracted tooth are of normal color or slightly hyperemic, the socket is filled with a blood clot, and the process of epithelization is in progress. When palpating the gums, a protrusion in the area of the edge of the socket or mobility of a fragment of the edge of the socket is determined. Sometimes the protruding edge of the interradicular septum may be palpable. Palpation of the listed formations causes pain.
Treatment of alveolar pain
Treatment of alveolar pain is carried out under local infiltration anesthesia. Treat the surgical area with an antiseptic solution. Using a narrow thin rasp, the gums are moved away from the alveolar edge, creating access to the edges of the alveoli. If a movable fragment of the alveolar edge associated with the gum is discovered, it is removed. The edges of the alveoli are examined and palpated, using a sharp curettage spoon or bone nippers, bone protrusions are removed and the edges of the alveoli are smoothed. If there is a protruding interradicular septum, it is partially removed using bone pliers. The surgical wound is treated with an antiseptic solution, and the gum is placed in its original place. In the absence of inflammation, the edges of the gums can be brought together with a suture. In the presence of inflammatory phenomena, solcoseryl can be injected into the alveoli in the form of a gel. A gauze swab soaked in an antiseptic solution is applied to the surgical area for 20-30 minutes.
The patient is prescribed analgesics and applications with a warm herbal decoction.
Prevention
Prevention of the development of this complication is the removal of the protruding edges of the alveoli, interdental and interroot septum directly during the tooth extraction operation.
Alveolitis
Alveolitis is a purulent infectious-inflammatory process in the periodontium of an extracted tooth. This is inflammation of the tooth socket, a widespread disease, which, according to various authors, accounts for 24–35% of the total number of all complications after tooth extraction.
Causes of alveolitis
The causes of alveolitis are traumatic tooth extraction, the presence of an inflammatory focus at the time of surgery, the presence in the wound of foreign bodies, fragments of roots and bone, granulation tissue in the periapical area, pushing infected dental plaque into the wound, the absence of a blood clot in the socket or its mechanical destruction if the patient does not comply postoperative regimen.
Clinical picture of alveolitis
Clinical picture of alveolitis:
- The leading symptom of alveolitis is pain, which appears or intensifies on the 3-4th day after tooth extraction. The pain is intense and constant, disrupting sleep and appetite.
- The general condition of the patient is disturbed due to debilitating pain and sleep disturbances.
- Low-grade fever and tachycardia corresponding to body temperature may be observed.
- The air exhaled by the patient has a putrid odor.
- The gums around the alveolus of the extracted tooth are hyperemic, swollen, and in places covered with fibrinous plaque.
- The alveolus of an extracted tooth may not contain a blood clot (“dry” alveolus), or may be partially filled with a loose gray clot. The walls of the alveoli are covered with a gray-dirty coating, its edges can rise above the gum.
- Regional lymph nodes are often enlarged, ovoid in shape, elastic in consistency, mobile, and painful on palpation.
Treatment of alveolitis
Treatment of alveolitis is based on anti-inflammatory therapy, removal of the disintegrated part of the clot from the tooth socket, fragments of the root, crown and creating conditions for tissue regeneration.
After local anesthesia has been performed, they proceed to treatment of the hole. Using a syringe with a blunt needle, a stream of warm antiseptic solution (hydrogen peroxide, furatsilin, chlorhexidine, potassium permanganate) is used to wash out particles of a disintegrated blood clot, food, and saliva from the tooth socket. Then, using a sharp surgical spoon, carefully remove the remains of a blood clot, granulation tissue, bone fragments, and teeth. After this, the hole is again treated with an antiseptic solution, dried with a gauze swab, powdered with anesthetic powder and covered with a bandage made of a narrow strip of gauze soaked in iodoform liquid, or an antiseptic and anesthetic dressing “Alvogyl” is introduced. BAP, a hemostatic sponge with gentamicin or kanamycin, and antibiotic pastes are used as a bandage on the hole. The bandage protects the socket from mechanical, chemical and biological irritants, while simultaneously acting antimicrobial.
Proteolytic enzymes
To cleanse the tooth socket from necrotic decay, proteolytic enzymes (trypsin, chymotrypsin, chymopsin) are used, which are dissolved in an isotonic solution of sodium chloride or in a 0.25% solution of novocaine (10 mg of enzyme in 5-10 ml of solvent). Enzyme therapy shortens wound healing time. The tooth socket can be filled with turunda with hydrophilic ointments (levosin, levonorsin, levomekol, miramistin, oflocaine, streptonitol, nitacid or 2% thiotriazoline) or moistened with an antiseptic solution (dioxidin), curiosin.
When treating alveolitis in patients with diabetes, it is recommended to inject turunda soaked in a solution consisting of 20 units of insulin, 5 ml of furatsilin 1: 5000 and 1 ml of a 5% solution of vitamin B1 into the cavity of the tooth socket.
Novocaine blockade of the mandibular nerve
Regional novocaine blockade of the mandibular nerve has a beneficial effect on the clinical course of alveolitis of the lower jaw. In general, all manipulations in the treatment of alveolitis must be carried out under local anesthesia, since the latter, in addition to the analgesic effect, has a beneficial effect on the course of the inflammatory process. For alveolitis, one of the types of physiotherapeutic treatment is used: fluctuarization, helium-neon infrared laser rays, local ultraviolet irradiation, magnetic therapy. Fluctuarization has an analgesic and stimulating effect. Laser therapy reduces vascular permeability, improves microcirculation, and provides analgesia. Irradiation of the hole with ultraviolet light has a pronounced antimicrobial effect. Magnetic therapy has an analgesic and anti-edematous effect. Non-steroidal anti-inflammatory drugs or analgesics are prescribed according to indications.
Prevention of alveolitis
In order to prevent alveolitis, the doctor must:
- Before tooth extraction, perform professional oral hygiene for the patient;
- comply with all successive stages of tooth extraction;
- make a revision of the hole, removing fragments of tooth and bone, bringing its edges closer together;
- when removing two or more adjacent teeth, apply sutures to the mucous membrane;
- carefully perform hemostasis;
- if there is no blood in the hole, fill it with iodoform turunda;
- recommend that the patient, after tooth extraction surgery, follow recommendations on diet and mouth rinsing.
The article was written specifically for the OHI-S.COM website. Please, when copying material, do not forget to provide a link to the current page.
Complications after sedation
Do nausea and fainting occur after sedation, or can such nuances be clarified before it begins? Of course, the characteristics of patients may be different: for some it may be nausea, for others it may be dizziness, etc. All this, of course, is discussed in advance in consultation with an anesthesiologist-resuscitator. It determines the patient’s health characteristics and determines the reactions that are possible due to the action of the drug. Any sedative drug can cause:
- drowsiness throughout the day after the manipulation, especially if the treatment was carried out in the morning,
- weakness,
- mild nausea
- It may make some people feel hungry, while others may feel the opposite.
There may be peculiarities, and this is not something pathological or something negative, this is the norm.
General anesthesia in dental practice
General anesthesia in dentistry is rarely used, mainly when it is necessary to carry out complex interventions in maxillofacial surgery, as well as in prosthetics. The drug is administered intravenously or by inhaling its vapor through a special mask. In order to treat teeth under general anesthesia, it is necessary to undergo a number of tests, such as an ECG, a general blood test, for hepatitis and HIV, and also consult an anesthesiologist.
Before manipulation, you should make sure that the patient is healthy to avoid possible complications.
Indications for this method of pain relief are:
- Intolerance to drugs used as local anesthesia.
- Panic fear of dental procedures.
- Mental pathologies.
Contraindications to this type of anesthesia:
- Diseases of the respiratory tract in the acute stage.
- Heart failure.
- Recent myocardial infarction.
- Drug or alcohol intoxication.