Perforation of the maxillary sinus during sinus lift is a complication that occurs during surgery to augment the bone tissue of the upper jaw . It is possible due to insufficient diagnosis, the use of outdated techniques, or the operation being performed by an inexperienced surgeon. As a result of undetected perforation, sinus inflammation and sinusitis develop, disturbing patients.
For more than 20 years, the Doctor Levin Center has been providing care to patients with complications after unsuccessful operations in the area of the maxillary sinuses. Surgical treatment is carried out in a specialized ENT department with modern equipment; operations are performed by maxillofacial surgeons with ENT training.
Causes of sinus perforation during sinus lift
Sinus lift is an operation to restore the bone tissue of the upper jaw. It is carried out in case of its deficiency in order to create sufficient volume for reliable fixation of the implant. Unlike other types of bone grafting, it has its own peculiarities - it is performed on the border with the maxillary sinuses, which are separated from the oral cavity by a thin bone plate.
During surgery, the sinus lining is separated from the periosteum, lifted, and the space is filled with bone material. At this moment, there is a risk of perforation if the surgeon has not previously conducted an extensive diagnosis, does not have sufficient experience and qualifications, or performs the operation using outdated equipment. The risks increase if the patient naturally has large and thin-walled sinuses.
- Open sinus lift
- Closed sinus lift
- Simultaneously with implantation
- Swelling after sinus lift
Diagnostics
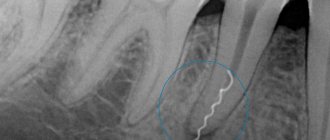
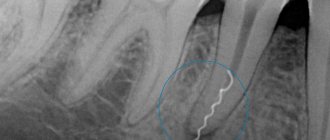
Determining the presence of the fistula itself is not difficult. To assess its depth and diameter, it is possible to use a special probe inserted into the resulting oroantral tract. To assess the extent of inflammation and the presence of additional passages, it is possible to use radiography of the upper jaw with the introduction of a contrast agent.
Evaluation of the presence of a foreign body or apex of the tooth root is carried out during radiography or directly during the operation to close the fistula. If there is no effect from antibacterial therapy, it is possible to culture the microflora to determine its resistance to antibiotics of various types of action.
How to prevent perforation
Perforation is possible even with full and proper compliance with the sinus lift protocol. However, it is not difficult to eliminate the risks if a detailed diagnosis is carried out before bone augmentation. In our Center, the examination is carried out on a modern SIRONA-SIEMENS 3D tomograph with the GALILEOS diagnostic software complex with ENT mode settings. Allows you to identify individual parameters:
- structural features of the jaw
- sinus condition
- bone density and size
- identify possible risks
- choose the most appropriate protocol for the upcoming operation.
It’s good if the clinic has software for 3D planning of the operation - it allows you to build a model of the jaw and perform a virtual operation, taking into account vulnerable areas.
This reduces the time of the actual procedure and eliminates risks. Not every dentistry is equipped with modern equipment; operations are carried out “the old fashioned way” using a “hammer and chisel”, when the risk of sinus perforation is quite high and you can only rely on the experience and qualifications of the surgeon. Such punitive methods are becoming a thing of the past in modern clinics. We use a low-impact ultrasound protocol . The piezo device delicately affects the bone, and when it approaches soft tissues - membrane, nerves, blood vessels, it turns off.
In approximately 5% of cases, the situation is provoked by unskilled actions of an inexperienced surgeon. Rest assured that a similar situation will not happen at the Doctor Levin Center. Operations in our Center are performed only by maxillofacial surgeons with ENT training . These are highly qualified doctors, candidates of medical sciences, with excellent clinical thinking and honed manual skills.
The likelihood of errors in our Center
is reduced to zero.
We have eliminated the risks of medical errors at every stage, and we work in accordance with the Center’s Unified Quality Standards. Our surgeons do not work “on the fly”; they provide dental care taking into account the characteristics of each clinical case, without restrictions on the time of patient appointment.
Levin Dmitry Valerievich Chief physician and founder of the Doctor Levin center
What to do if perforation does occur
After studying the CT image, the surgeon must be prepared for any emergency situation. If a sinus perforation does occur, it is important to immediately resort to microsurgery to close the hole. Otherwise, infection and inflammation of the sinus and the development of complications are possible.
- If the hole diameter does not exceed 2 mm , the perforation heals without surgical assistance. The progression of rupture is prevented by fixing the membrane.
- A perforation measuring 2-4 mm requires emergency closure. Sinus lifting continues after suturing - this is enough to prevent infection.
- A perforation of more than 4 mm is a reason to terminate the sinus lift. The procedure can be carried out only after the hole has healed.
An experienced doctor will always understand that the operation did not go according to plan and will take immediate measures to prevent complications.
Self-healing of a hole with a diameter of more than 2 mm with bone tissue is impossible! Emergency surgical closure of the anastomosis is required.
Signs if the situation was left without the attention of a doctor
Even if the surgeon is inattentive, the patient will suspect perforation on his own soon after the operation:
- There is yellowish or bloody mucous discharge from the nasal passages
- Feeling strange smells and tastes in the nose and mouth
- The voice becomes nasal and the timbre changes
These are primary symptoms that may gradually disappear. But if they are left unattended, the situation becomes more complicated. As a result of the infectious-inflammatory process, the soft and hard tissues of the alveolar process and the maxillary sinus melt, and a fistula is formed - a pathological passage between the oral cavity and the sinus, which interferes with the healing processes.
The situation is aggravated when bone material enters the maxillary sinus if the surgeon has not installed a barrier membrane. After a while, inflammation begins around the foreign body, and secondary infections occur. The process spreads to surrounding tissues.
Sinus inflammation can occur in a latent form and not bother the patient for several years. But sooner or later the process is activated, and signs of sinusitis appear - pain, swelling, nasal congestion. The sinus is susceptible to inflammation from the side of the sinus lift . An attentive patient will pay attention to this and find a connection with the operation.
Material and methods
Materials on this topic published over the past 13 years (from 2000 to 2013 inclusive) were used. The database search was carried out using keywords: odontogenic maxillary sinusitis, odontogenic sinusitis, odontogenic maxillary ethmoiditis, oroantral fistula repair, oroantral communication, OAC, OAP, OAF, oroantral
,
antroora
,
orosinusal
,
communication
,
fistula
,
perforation
, etc., as well as their combinations.
Etiological features and classification
The presence of an oroantral communication is the main etiological factor in the development of the perforated form of odontogenic maxillary sinusitis [3]. The etiological significance of perforations according to Russian authors is estimated at 60-95% [3]. 41.2–77.2% of odontogenic sinusitis are its perforated forms [1]. According to foreign sources, communication between the oral cavity and the maxillary sinus occurs after tooth extraction with a frequency of 0.31 to 4.7% [4].
Perforation of the maxillary sinus is more common in male patients than in women [5]. The prerequisites for the occurrence of perforation are: 1) anatomical features of the sinuses and alveolar process of the upper jaw; 2) the presence of an odontogenic inflammatory process that contributes to the thinning and destruction of bone tissue; 3) errors in tooth extraction and management tactics for such patients. Anatomical features that contribute to the occurrence of communication include the pneumatic type of structure of the sinuses, a thin cortical bone plate and the protrusion of the roots of the teeth into the cavity of the maxillary sinus [6-10]. Perforated sinusitis in most cases occurs when molars (less often premolars) of the upper jaw are removed due to various forms of chronic periodontitis [3, 7—9]. Odontogenic maxillary sinusitis can be a complication of unsuccessful sinus lift surgery, especially in patients with severely thinned cortical bone [11].
Research by A.I. Bogatova [7] found that the source of infection of odontogenic sinusitis most often (56.6%) is the first molar.
At the same time, an important role is played by the structure of the ostiomeatal complex (paradoxically curved middle turbinate, enlarged ethmoidal bulla, expanded, curved pneumatized, uncinate process) and obstruction of the natural anastomosis of the maxillary sinus, leading to difficulty in the outflow of contents from the maxillary sinus and the development of the inflammatory process [8 ].
Oroantral messages in perforated odontogenic maxillary sinusitis can be classified according to the time of occurrence of the message, location, and size of the defect.
The following types of perforations are distinguished: 1) accidental and suspected; 2) recognized and unrecognized; 3) complicated and uncomplicated; 4) perforation, in which the causative tooth is removed, or not removed, or partially removed [9].
Perforations of the maxillary sinus, including post-extraction ones, are also divided according to the course of the process into acute and chronic. The first are discovered during dental surgery or immediately after its completion. Chronic perforations of the sinuses can be detected several days after tooth extraction [8, 9].
There are perforations of point, slit-like, round, oval and irregular shapes of various diameters. They can be localized outward from the alveolar process, i.e., in the vestibule of the oral cavity, on the alveolar process and from the inside of it, on the palatal side.
Accordingly, alveolar sinus, palatosinus, vestibulosinus [5, 9] perforations are distinguished.
Oroantral communication plastic surgery
It is advisable to divide the tactics of treatment of odontogenic maxillary sinusitis with oroantral communication into several stages depending on the timing of its occurrence.
In the event of spontaneous occurrence of oroantral communication (for example, during extraction of a diseased tooth) and the absence of severe inflammation of the sinus mucosa, in order to prevent the development of sinusitis, a blood clot is usually preserved in the socket of the extracted tooth [4, 9]. According to A. Borgonovo [5], spontaneous oroantral communications less than 3 mm without infection and without epithelization of the fistulous tract should be treated immediately, or at least within 24-48 hours [5]. According to S. Visscher et al., Gacic et al. [4, 12], defects up to 2-5 mm can close on their own. For formed epithelialized oroantral fistulas larger than 5 mm and lasting more than 3 weeks, fistula repair is necessary [8, 12].
Many authors note that in case of spontaneous perforation of the sinus, it is considered advisable to tamponade the lower third of the tooth socket with an iodoform tampon, a hemostatic sponge, or a loose tamponade for 5-7 days for better preservation and organization of the clot [4]. It is possible to fix tampons with thin wire using an aluminum dental splint, protective plates made of tantalum or various plastics [9].
Successful wound closure has been described using fibrin glue, fibrin film, stabilized blood clot, and histocryl tissue adhesive [4, 8, 9].
In the presence of a persistent, formed oroantral fistula, prolonged inflammation of the mucous membrane of the maxillary sinus, the presence of periodontitis, damage to the bone of the alveolar process with signs of productive inflammation (presence of granulations, cysts, osteoporosis) are noted, as a result of which OPVS is considered a primary chronic disease [7, 9, 13].
Traditionally, with OPWS, as with rhinogenic maxillary sinusitis, the patient undergoes radical surgery on the maxillary sinus with further opening of the ethmoidal labyrinth cells, the imposition of an anastomosis with the nasal cavity according to Caldwell-Luc and plastic surgery of the oroantral communication with a mucoperiosteal flap [14, 15].
It should be remembered that after radical surgery on the maxillary sinus, relapses, formation of scar tissue, sclerotic changes in the walls of the sinus, sinus collapse, formation of postoperative cysts of the upper jaw, “disease of the operated sinus” are possible [8, 15, 16].
In light of the modern development of endoscopic technologies and the desire of rhinosurgeons for more gentle surgical interventions, endonasal surgical interventions and endoscopic micromaxillary anastomies with revision of the natural anastomosis are currently performed. With these interventions, it is possible to reduce trauma to the walls of the sinus, especially the anterior (facial) wall [15-19].
There is an opinion that with isolated odontogenic maxillary sinusitis, i.e. with changes in only the lower (alveolar) wall with a wide natural sinus anastomosis, no signs of damage to other walls and without damage to the ethmoidal labyrinth, it is possible to perform a maxillary sinusotomy with removal of the mucous membrane only on the lower wall and subsequent repair of the fistula [9].
However, it should be noted that all patients with clinical manifestations of diseases of the paranasal sinuses should undergo nasal endoscopy, since the predominant part of acute, recurrent and chronic sinusitis has rhinogenic causes [18].
According to domestic and foreign authors, radical removal of a functionally complete mucous membrane leads to disruption or absence of mucociliary clearance [9, 15]. However, according to research by V.T. Palchun and E.B. Vladimirova [20], the sinus mucosa is restored after radical surgery on the maxillary sinuses.
Methods for plastic surgery of persistent formed alveolar fistula are divided into 4 types: vestibular flap, alveolar flap, buccal flap, combined type. These types with movement and rotation of the flap are used to close defects larger than 5 mm in diameter [12].
Most often, surgeons use vestibular and buccal flaps of a trapezoidal shape with a base in the area of the transitional fold, which, after mobilization, is sutured to the edges of the defect [12].
Methodology V.V. Skorobogaty [13] involves exfoliation of the mucous membrane in order to expose the canine fossa, forming a periosteal-osseous-mucosal flap on the anterior wall of the sinus [13].
The disadvantage of vestibular flaps is deformation of the vestibule of the oral cavity, which subsequently complicates dentures [5, 12]. Modification of fistula repair according to S.Z. Piskunov, T.G. Bykanova provides double-layer closure of the perforation with a mucoperiosteal flap [9, 21].
A.A. Limberg used a flap cut from the side of the hard palate, which is quite thick and well vascularized due to the superior great palatine artery. The disadvantage of this technique is the long healing of the hard palate wound by secondary intention, the need to manufacture and wear a protective plate on the palate, as well as the high probability of necrosis (cited from [9, 10]).
For small fistulas, the edges of the wound around the fistula opening are excised, two parallel incisions are made running from the vestibule of the mouth to the palatal side, hemostasis and suturing of the mucous membrane over the fistula are made.
Methods for closing the alveoli with a cheek flap containing fatty tissue are also described. Such flaps should be used for large perforations localized in the posterior parts of the alveolar process. However, for a long time this flap was little used due to possible trauma to the pterygomaxillary space. H. Tideman (cited from [12, 22]) described in detail the anatomy, vascularization and surgical technique of using a buccal flap with a fat “cushion”, known as Bichat’s lump. The advantage of using this technique is the epithelization of the buccal flap with a Bichat lump in a shorter time.
The available literature describes methods for taking a distal flap from the lateral or posterior surface of the tongue [12]. The lingual flap, like the palatal flap, has good vascularity and is convenient for closing large oroantral communications. The disadvantage of the lingual flap is that it is traumatic and requires additional anesthesia, as well as the presence of a so-called “second” surgical field.
It is possible to use a combined method of closing perforation of the floor of the maxillary sinus through the combined use of tissues taken from the vestibule of the oral cavity and from the hard palate [9].
It is worth noting that immediate plasty of spontaneous oroantral communication without signs of inflammation of the maxillary sinus, according to statistics, is more successful (95%) compared to plasty of long-term persistent oroantral fistula (67%) [12].
In all cases of plastic surgery, the flap should be positioned without tension, and the suture line should be on the bone base [9].
However, despite the fairly low percentage of fistula recurrences (from 5 to 15%, according to G.B. Troshkova), plastic surgery of the oroantral communication with only a mucoperiosteal flap does not solve the problem of a bone defect in the lower wall of the maxillary sinus and excludes the possibility of further dental implantation in this area and carrying out comprehensive rehabilitation of patients (cited from [9]).
Currently, the literature describes many methods for eliminating a bone defect with autografts and osteoplastic materials for odontogenic maxillary sinusitis.
Osteoplastic materials used to close an oroantral fistula can be divided into autogenous, allogeneic, xenogeneic, synthetic, etc.
In modern dental osteoplasty, the first place when choosing a material is not just the rational replacement of a bone defect, but the severity of the inductive potential of the material - its ability to form full-fledged bone [23].
Autografts (genetically identical materials) certainly have a high inductive potential. In the literature, there are examples of using a fragment of the medial and anterior walls of the maxillary sinus for plastic surgery of small oroantral communications. For larger defects spina
iliaca anterior superior
, a rib, and material from the zygomatic process, mental region, body and ramus of the mandible were used [12, 24-26]. R. Haas [26] took a bone fragment from the chin area using metal screws to fix the bone. He recommends this localization of material sampling for atrophy of the upper jaw to enlarge the sinus. Y. Kitagawa et al. [27] successfully transplanted a third molar into the socket area with oroantral communication. The disadvantages of autografts include the presence of a donor zone, i.e., two surgical fields - additional trauma to the patient, limited volume of the necessary plastic material, and the complexity of its extraction. It should be noted that proximally taken autogenous implants are preferable to distal ones, since they reduce the time required to isolate bone fragments and also do not cause postoperative discomfort in the patient.
Allogeneic implants
(genetically different materials from the same biological species) have an inductance comparable to autogenous implants. However, for the presented group of materials it depends on the methods of processing, technical production and preservation of materials.
To close the oroantral fistula in odontogenic maxillary sinusitis, materials such as fibrin glue in combination with collagen plates, preserved dura mater, lyophilized dura mater with a plastic plate for fixation, embryoblast, demineralized frozen dried bone matrix, preserved amnion with subsequent fixation with catgut are used. suture to the circular ligament of the tooth socket [8, 9, 12].
A significant disadvantage of allografts is the possibility of allergic reactions caused by the lack of compatibility of donor and recipient tissues. Other disadvantages are the problem of patient infection with hepatitis virus, HIV, as well as the problem of procurement and storage of materials.
Xenogeneic implants
(materials from another biological species) - materials representing natural hydroxyapatite, which has preserved the bone structure after the removal of proteins to which an immunological reaction may develop. For these purposes, cattle bones that have undergone chemical and heat treatment are used. An example is the material Bio-Oss, Osteograph/N.
Synthetic osteoplastic materials
are inert materials (Interpor, Osteograph/D, Durapatite) - a replacement for natural hydroxyapatite, as well as neutral or inert implants that are used only to fill space. An example is various metals, such as gold, titanium nickelide, aluminum.
Absorbable materials provide a scaffold for bone formation but do not induce osteogenesis, and hydroxyapatite can be replaced by newly formed bone.
Recently, composite osteoplastic materials are increasingly used in medical practice. For example, Kolapan, Kolapol consist of hydroxyapatite and collagen. It is believed that collagen has the ability to attract osteogenic cells and promote their attachment to the surface of hydroxyapatite [28].
M. Shaker closed the oroantral fistula with porcine collagen, followed by immediate covering of the communication with a buccal or palatal mucoperiosteal flap. In 29 out of 30 patients, a positive result was observed in the form of closure of the fistula and the formation of new bone (cited from [12]).
K. Thoma, G. Pajarola [29] reproduced the tooth root from B—
tricalcium phosphate using the mold of the extracted tooth. No complications were observed. However, this method requires precise alignment of the formed tooth root and the socket.
Guided tissue regeneration method
Directed tissue regeneration (contact suppression) is the ability of a material to prevent apical proliferation of the epithelium [23].
T. Waldrop et al. (cited from [12]) used the method of directed tissue regeneration to close oroantral fistulas using a gelatin membrane, an allogeneic bone fragment and a non-absorbable polytetrafluoroethylene membrane. The materials were sequentially placed into the perforated tooth socket and covered with a buccal mucoperiosteal flap. After 8 weeks, the polytetrafluoroethylene membrane was removed and, upon visual inspection, the identified full bone was again covered with a mucoperiosteal flap. The researchers did not perform histological analysis of the newly formed bone.
In recent years, more and more preference has been given to combined methods of closing the oroantral communication, consisting of osteoplastic material and a membrane of directed tissue regeneration.
According to the literature, the osteoplastic material Bio-Oss occupies a leading position on the market.
C. Ogunsalu [30] used the “sandwich” technique, suturing two Bio-Gide membranes together with an atraumatic absorbable vicryl thread on three sides, placing granules of the Bio-Oss osteoplastic material inside and suturing them on the fourth side, so that a closed “sandwich” was obtained. After which a buccal trapezoidal mucoperiosteal flap was cut out. A “sandwich” was placed in the area of the oroantral opening, the convex side of which faces the bottom of the sinus, and the concave rough side faces the oral cavity. The remains of the osteoplastic material and then the mucoperiosteal flap were placed on top. The author considers this technique promising, since he received a positive result in the form of the formation of a sufficient volume of alveolar bone tissue for further dental implantation.
A.A. Nikitin et al. [1] performed an osteotomy of the vestibular bone plate of the alveolar process in the projection and at the level of the boundaries of the oroantral anastomosis. The osteotomized bone fragment with the mucous membrane attached to its inner surface was displaced into the cavity of the maxillary sinus. The mucosal defect in the area of the bottom of the maxillary sinus was sutured with atraumatic absorbable vicryl sutures. The alveolar process defect was filled with Bio-Oss biocomposite material and isolated from the mucous membrane with a Bio-Gide membrane. A previously isolated trapezoidal mucoperiosteal flap from the cheek was placed on top. After 6 months, the authors noted sufficient bone volume in the alveolar process.
The study by Yu.M. is of interest. Pogosyan [31], in which the closure of the oroantral fistula was carried out using a beeswax membrane, platelet-rich blood plasma in combination with allogeneic bone material. There were no complications associated with the use of this method of oroantral fistula repair.
Why you should entrust treatment to the ENT department of dentistry
ENT dentistry combines two types of medical services - otolaryngology and dentistry. This is a comprehensive approach to the treatment of complications after surgical operations performed on the upper jaw in the area of the maxillary sinuses.
Our Center specializes in providing assistance to patients who find themselves in difficult situations. Often, before coming to our clinic, patients unsuccessfully run with symptoms of sinusitis from the otolaryngologist to the dentist in a vicious circle. Only maxillofacial surgery with ENT training is able to identify the problem and draw up an adequate treatment plan.
Treatment in the ENT Department of Dentistry is indicated in cases where:
- old perforation after sinus lift
- inflammatory processes in the maxillary sinus
- presence of bone replacement material
- attached neoplasms
Consequences and prevention of injury
This complication, if left untreated, can lead to:
- inflammation of the maxillary sinus;
- infection of surrounding bone tissues with transition to other sinuses of the skull;
- formation of foci of osteomyelitis in the upper jaw;
- suppuration of foci of infection;
- loss of healthy teeth in the affected area.
If the perforation was not identified and treated in time, this can lead to the development of sinusitis or acute sinusitis, which is characterized by acute pain, swelling of the nasal mucosa - with difficulty breathing and purulent discharge.
To avoid such unpleasant consequences of dental treatment for the patient, specialists at the Implantmaster clinic conduct a comprehensive study of the patient’s anatomical features using X-ray and computed tomography images and strictly observe the accuracy of medical manipulations.
Branded rehabilitation
For those who want to recover faster, we offer an accelerated rehabilitation program - quickly relieves swelling and eliminates bruises
Injection procedures are performed immediately after surgery while the patient is still under sedation. Physiotherapy procedures are usually prescribed on the third day, when postoperative discomfort worsens and the patient understands what difficulties he has.
Microcurrent therapy
Pulsed low-frequency currents restore metabolism at the cellular level. Relieves swelling, muscle spasms, reduces hematomas.
PRP plasma therapy
Injections of enriched blood plasma increase the ability of cells to regenerate, lymph and blood flow. Minimize swelling and cosmetic defects.
Biostimulation of the face
Biomodulators D-NUCLEO and MesoSculpt C71 accelerate recovery, have a lymphatic drainage effect, an anti-inflammatory effect, and reduce swelling.
Recovery period
Home medication is prescribed - a course of antibiotics and anti-inflammatory therapy. To prevent the patient from running to pharmacies in a postoperative state and to avoid purchasing uncertified products, we provide the entire package of necessary medications free of charge .
The medicine package contains a detailed list of recommendations and a card with a 24-hour support number.
The service operates 24/7 , if you have any problems, call the number provided.
After 10-14 days, the patient is invited to have the stitches removed. A follow-up CT scan is performed and an examination date is set to monitor the situation.
Treatment of damage to the maxillary sinuses
Treatment is determined by the degree of damage, the presence of foreign bodies in the cavity, as well as the speed of diagnosis and initiation of treatment. The only non-surgical treatment is one that was diagnosed at the time of tooth extraction and does not have signs of infection or the presence of foreign bodies in the sinus. In this case, the doctor does everything to keep the blood clot that closes it in the tooth socket and prevent it from becoming infected. For this purpose, a gauze swab soaked in iodine solution or a special plastic plate is placed in the hole; in rare cases, sutures are required.
These dental procedures are performed in combination with a course of antibiotics, drops with a vasoconstrictor effect and anti-inflammatory drugs. If a foreign object gets inside the maxillary cavity, treatment is carried out surgically through opening and removal of the foreign object and non-viable tissue. The specialists of the Implantmaster clinic not only effectively treat such injuries, but also do everything possible so that their patients know about them only by hearsay.