Technique of torusal anesthesia
1. The patient opens his mouth as wide as possible (Fig. 101, B). Injection site: the intersection point of a horizontal line drawn 5 mm below the chewing surface of the third upper molar with the groove formed by the lateral slope of the pterygomaxillary fold and the cheek. 2. The syringe is located on the first lower molar (or even on the second lower molar), the needle is directed perpendicular to the plane of the mandibular ramus.
Rice. 101. Torusal anesthesia according to M.M. Weisbrem (S.N. Weisblat, 1962). A - diagram of the location of nerves in the area of the mandibular eminence: 1 - buccal nerve; 2 - lingual nerve; 3 - inferior alveolar nerve; 4 - mandibular eminence (torus); 5 - a horizontal line drawn 5 mm below the chewing surface of the third upper molar (reaches the torus). B — position of the needle injection, position of the syringe during torusal anesthesia
3. The needle is advanced into the soft tissue to the bone to a depth of 15-20 mm, an aspiration test is performed, 1.5-2 ml of anesthetic is injected, anesthetizing the inferior alveolar and buccal nerves. 4. Having advanced the needle a few millimeters, 0.3-0.5 ml of anesthetic is released to anesthetize the lingual nerve. Anesthesia occurs within 3-5 minutes. Note : In the last 3 years, using modern strong anesthetics, we have not advanced the needle to anesthetize the lingual nerve (point 4). When 1.5-2 ml of anesthetic is injected near the bone, the anesthesia zone covers both the inferior alveolar, buccal and lingual nerves. 5. Anesthesia zone : the same tissues as with mandibular anesthesia, as well as: mucous membrane and skin of the cheek, gums of the lower jaw from the middle of the second premolar to the middle of the second molar on the vestibular side. 6. Complications are the same as with mandibular anesthesia.
Medical Internet conferences
To motivate children for timely dental treatment, it is necessary that all interventions in the dental chair are minimally painful. This can only be achieved with high-quality anesthesia. In pediatric dental practice, of all types of anesthesia, infiltration, mandibular, torus and palatal anesthesia are most often used. In the lower jaw, mandibular anesthesia is often used, in which the inferior alveolar and lingual nerves are switched off. The area of anesthesia is: the mucous membrane and periosteum of the alveolar process on the lingual side on half of the jaw; anterior 2/3 halves of the tongue; half of the lower lip; all teeth on the corresponding half of the lower jaw: mucous membrane and periosteum on the vestibular side of the alveolar process, except for the area near the molars, which requires additional infiltration anesthesia, since this area is innervated by the buccal nerve. Fig.1.
Knowledge about the features of mandibular anesthesia is significant when planning measures to provide emergency care in emergency conditions and in the treatment of surgical pathology in children, therefore, during its implementation, you should know the following landmarks or features: the location of the bone tongue and the mandibular foramen on the medial surface of the lower branch jaws. There are anatomical differences in the size and proportions of the bones of the maxillofacial region in children, which must be taken into account when administering anesthesia.
In a 3-5 year old child, the mandibular tongue is located approximately at the level of the occlusal surface of the teeth; with age, the position of the tongue changes upward and posteriorly relative to the occlusal plane, and already in a 15-16 year old teenager it is located approximately 1 cm above it (as in an adult) , therefore, when carrying out anesthesia, the needle is injected not 1 cm above the chewing surface of the lower molars, as in adults, but at the level of the chewing surface of these teeth and the lower the younger the child.
The branch of the lower jaw in children 3-5 years old is twice as narrow as in an adult; the volume of the pterygomaxillary space in children is less than in adults, therefore the mandibular, lingual and buccal nerves are located closer to each other. The angle of the lower jaw in an infant is 140º-145º, due to which the mandibular foramen itself is located lower, being in the same plane with the chewing surface of the lower molars. With age, the angle of the lower jaw decreases due to the eruption of permanent teeth, including wisdom teeth. In preschool children, the needle penetrates soft tissue by 10-15 mm (in adults by 15-25 mm). Therefore, children are given pain relief with a short needle. For anesthesia of the inferior alveolar nerve, 0.5-1 ml is enough for children. anesthetic (adults 1.5-1.8 ml). In preschool age, using mandibular anesthesia, it is often possible to turn off the sensitivity of all three nerves (inferior alveolar, lingual, buccal) that innervate the teeth of the lower jaw, which makes it possible to use additional anesthesia of the buccal nerve less often.
In accordance with the growth of the jaws, the change in the location of the mandibular foramen has the following patterns: Fig. 2. In children 3-5 years old it is located 1-2 mm below the chewing surface of the teeth of the lower jaw, and in children over 6-8 years old - at the level of the chewing surface of these teeth, in children 9-11 years old - 3-5 mm higher level of the chewing surface of these teeth, 12 years and older - as in adults - 1 cm above the level of the chewing surface of these teeth.
Based on the above, it follows that mandibular anesthesia at different ages is carried out taking into account the anatomical features of the structure of the jaws, ignorance of which can lead to poor quality anesthesia and, consequently, to more painful necessary manipulations. As a result, the young patient is left with a negative memory of the dental appointment and a reluctance to be observed and treated in the future, which leads to the more frequent occurrence of advanced diseases.
Technique of “high” anesthesia of the inferior alveolar nerve
Carrying out standard mandibular anesthesia does not always provide sufficient anesthesia of the lower jaw, which can be explained by the presence of additional innervation. The teeth of the lower jaw can receive additional innervation from the hypoglossal, auriculotemporal and upper cervical nerves. The hypoglossal branch leaves the trunk of the inferior alveolar nerve approximately 1 cm above the mandibular foramen and therefore cannot be switched off using conventional techniques. Branches from the auriculotemporal nerve extend to the pulp of the lower teeth through openings in the ramus of the lower jaw. This innervation is blocked by “high” anesthesia according to GAGow-Gates and JOAkinosi.
Anesthesia of the inferior alveolar nerve.
There are three levels of inferior alveolar nerve block. The lower block is standard mandibular anesthesia using the palpation method, the middle block is torsal anesthesia, and the upper block is Go-Gates anesthesia. These three methods of blocking the inferior alveolar nerve are used in different clinical cases. If mandibular anesthesia is ineffective, in order not to create an anesthetic depot in the same area, it is recommended to repeat higher methods of blocking the inferior alveolar nerve: torus anesthesia or Go-Gates anesthesia. If the patient has a history of unsatisfactory results of mandibular anesthesia, it is also recommended to use high blockade methods. On a toothless jaw, it is easier to perform torus anesthesia or Go-Gates anesthesia. When performing surgical interventions on lower molars, in the case of a local infectious process, it is better to use anesthesia that provides simultaneous blockade of the buccal nerve. In many cases, the choice of method for blocking the inferior alveolar nerve is a matter of the doctor’s habit or a feature of the school where his training was originally carried out.
a) Levels of mandibular nerve block; b) The place where the needle is inserted during local anesthesia.
Mandibular anesthesia by palpation.
Before administering anesthesia, the main bony landmarks of the mandibular ramus should be identified by palpation. These include the anterior edge of the jaw ramus and the temporal ridge, located somewhat inward.
Bone landmarks for mandibular anesthesia by palpation.
The needle is inserted medially from the temporal ridge, 1 cm above the occlusal surface of the lower molars. The syringe is located in the opposite corner of the mouth. The needle is advanced until it contacts the bone tissue, a depot of 0.3 ml of anesthetic is created, then the syringe is moved towards the opposite corner of the mouth and the needle is advanced backwards and outwards by 2 cm. An aspiration test is performed. An anesthetic depot of 1 ml is created. Among the positive aspects of this type of anesthesia, it should be noted that it is relatively easy to perform, because By palpation it is easy to determine the main bony landmarks. However, mandibular anesthesia is ineffective in 15 - 20% of cases. Mandibular anesthesia over the lower block does not provide anesthesia for the buccal nerve, so it is blocked separately by infiltrating a specific tooth. Due to the high density of large vessels in the distal part of the pterygomaxillary space, the frequency of positive aspiration tests is 12 - 15%. What are the reasons for the ineffectiveness of mandibular anesthesia? 1. Firstly, bony protrusions medially from the internal oblique line (temporal ridge) interfere with the reversal of the needle. 2. Secondly, anatomically, the mandibular foramen in some cases may be located slightly higher than 2 cm from the occlusal surface of the lower molars. In this case, mandibular anesthesia will be ineffective. Also, on a toothless jaw, due to the absence of lower molars as the main landmarks for the height of needle insertion, anesthesia will be difficult. H. In some cases, the innervation of the lower molars is carried out due to the additional branches of the maxillary-hyoid nerve (n. myelohyoideus). Mandibular anesthesia does not provide blockade of this nerve.
Torusal anesthesia.
The reference point for torsal anesthesia is the pterygomaxillary fold, which is formed by the anterior edge of the medial pterygoid muscle. The syringe is located in the opposite corner of the mouth. The needle is inserted 0.5 cm below the occlusal surface of the upper molars, outward from the pterygomaxillary fold. The needle is advanced anteriorly and outward until it contacts the bone tissue, and an aspiration test is performed. An anesthetic depot of 1.5 ml is created. This type of anesthesia provides anesthesia to the buccal, lingual and inferior alveolar nerves.
Anesthesia according to Go-Gates.
The purpose of anesthesia is to create an anesthetic depot in the area of the neck of the condylar process of the mandibular ramus. The main anatomical landmark during its implementation is the retromolar depression of the upper jaw, which is easily visible in normal and edentulous conditions. With the patient's mouth open as much as possible, the syringe is located in the opposite corner of the mouth, and the needle is inserted into the retromolar depression. The needle is advanced upward, posteriorly and outward, until it contacts the bone tissue of the neck of the condylar process. An anesthetic depot of 1.5 ml is created. An additional guideline for advancing the needle is a finger placed in the external auditory canal. That. the needle is advanced towards the finger. The patient is asked to make 10 open-close mouth movements. This type of pain relief is effective in 98% of cases. The rate of positive aspiration tests is less than 2%. Due to the fact that the soft tissues in the area of the neck of the condylar process are poorly vascularized, the rate of resorptive effect of the local anesthetic will be lower. It follows from this that the duration of anesthesia according to Go-Gates is much longer than with mandibular anesthesia. However, this method of anesthesia is difficult to perform due to the lack of clear guidelines.
Gau-Gates Method
The technique of this anesthesia is very complex and consists of creating an anesthetic depot near the head of the articular process of the lower jaw. 1. The patient opens his mouth wide. 2. The doctor draws a mental line from the corner of the mouth to the depression (pit) near the tragus of the ear. This is the plane in which the needle will advance. 3. The needle is inserted from the side of the opposite mandibular canine and directed through the medial palatal tubercle of the upper second molar located on the side of the anesthesia. 4. The needle is injected into the mucous membrane (the needle injection site is much higher than with conventional mandibular anesthesia) and deepened into the soft tissue towards the bone (to contact with the head of the articular process) (Fig. 102 A).
Fig. 102. Needle position for “high” blocking of the inferior alveolar nerve. A - according to the Gau Gates method. B - according to the Akinosi method.
5. The needle is slightly pulled back, an aspiration test is performed, and after injection, the entire contents of the syringe enter the soft tissue near the articular process. 6. The patient should keep his mouth open for several minutes until signs of anesthesia of the lower jaw appear.
Anesthesia in dentistry
One of the most common questions for adults and children when visiting a dentist is: will it hurt?
Most adult patients understand the times when treatment without pain was impossible due to the lack of anesthetics - drugs that provide anesthesia. It is this negative experience that prevents patients from being calm about dental treatment, both for themselves and their children.
However, we all understand that the less often we visit our doctor, the more problems we may have in the future.
Any qualified specialist will tell you that timely preventive visits to the dentist will be better both in terms of the activities carried out (for example, professional oral hygiene) and in terms of financial costs.
Modern medicine has already advanced far enough in the field of pain management to allow patients completely painless treatment, taking into account their state of health.
The essence of anesthesia itself (from the Greek “without feelings”) is the effect of medications on a certain area of your body or on the entire body as a whole.
Blocking the transmission of sensations along nerve fibers occurs by influencing a certain part of the nerve for which the corresponding part of the cerebral cortex is responsible, which causes a loss of sensitivity in it for the required time.
We use pain relief for:
- Treatment of caries of various depths, tooth depulpation;
- Surgical operations, incl. tooth extraction, implantation, bone grafting, soft tissue grafting, etc.;
- Orthopedic treatment that requires pain relief at certain stages, for example when treating a tooth for a crown or when placing it and the presence of discomfort in the patient;
So, let's figure out what types of anesthesia are distinguished, that is, let's discuss the classification of the methods used:
That is, the general division implies anesthesia carried out by applying or injecting anesthetics and anesthesia affecting the entire body as a whole.
Accordingly, in the first case, the patient is conscious, and we block the pain in the area we need by direct impact on it.
And in the second case, we use the intravenous or inhalation method of administering anesthetics to put the patient into a medicated sleep.
Also, separately, as a method of preparing for the main type of anesthesia that will be used, we sometimes use premedication methods, that is, psychological and medicinal preparation.
For example, if you feel afraid before visiting a doctor, you can make yourself a “cocktail” of valerian and motherwort! If you have an inflammatory process that requires tooth extraction or other surgical intervention, you can ask your doctor about the need to start taking antibiotics and anti-inflammatory drugs before the procedure itself.
We all know what nitrous oxide is, which is widely used in the field of pediatric dentistry and helps us and our children be treated in comfortable conditions and dance during tooth extractions and canal treatment; but this is also a way of premedication - preparation and assistance in the treatment process!
And yet, let’s return to our topic, let’s talk about the types of local anesthesia.
- Applique.
- Infiltration.
- Conductor.
- Intraligamentary.
- In-canal.
- Intraosseous.
- Stem.
They are arranged according to the frequency of use, from the most used to the rare species in everyday practice. Learn more about each of them.
Application anesthesia
This type is familiar to all, or most of our dear patients. We call it differently, most often fruit jam or pain-relieving gel for those who are older. It involves applying an anesthetic to the mucous membrane before the actual injection. Available in the form of gels, ointments or spray. Pain relief occurs quite quickly and during this period we already administer injection anesthesia.
You can also apply the gel to:
- relieving discomfort before treating mucosal wounds (stomatitis, gingivitis);
- when carrying out professional hygiene in particularly sensitive areas;
- when removing temporary teeth that have an extreme degree of mobility, that is, literally on the verge of falling out.
Infiltration anesthesia
The most used and loved by dentists is infiltration anesthesia. Provides numbness to the area and number of teeth we need during manipulation. The drugs used are ultracaine, mepivacaine, ubistezin, scandonest, each for its own case is selected individually at the appointment.
When you come to an appointment for the treatment of medium and deep caries, endodontic manipulations, removal of single-rooted teeth or simple surgical procedures, we perform this particular anesthesia.
Conduction anesthesia
We go according to the degree of increasing the strength of the anesthesia! Conduction anesthesia is so called because the trigeminal nerve is blocked by sending an anesthetic to the point where this nerve exits the bone.
Accordingly, all areas to which this nerve gives off its branches become numb. In this case, not only the zone of numbness increases, but also the duration of action of our anesthesia, up to 2-3 hours.
The scope of application is extensive, this is the removal of multi-rooted teeth on both jaws, incl. eights; therapeutic interventions on a large number of teeth at a time and individual increased sensitivity in patients requiring more serious pain relief.
Most often we use tuberal anesthesia in the upper jaw, which is performed in the area of the tubercle of the upper jaw and blocks part of the posterior branches of the nerve. In the lower jaw, in turn, torus anesthesia is used to block the inferior alveolar, buccal and lingual nerves.
Intraligamentary (intraligamentous) anesthesia
The name itself speaks for itself; the anesthetic is injected into the periodontal ligament itself (the fibers of which surround the tooth on all sides). This type is often used in children, because it makes it possible to locally numb the tooth without numbness of the lips and cheeks, because children can bite them after taking them.
Intraosseous anesthesia
It also has a rather self-explanatory name: the drug is injected first into the gum to numb it, and then deeper into the spongy layer of bone between the teeth. It is used in the absence of adequate pain relief from other types of anesthesia, for example, during tooth extraction surgery.
Trunk anesthesia
This type is unlikely to be familiar to you, since it is used in maxillofacial surgery hospitals during operations for injuries or damage to large areas. The anesthetic is applied to the base of the skull, blocking the transmission of nervous reactions along the maxillary and mandibular nerves. Of course, the duration and strength of action exceeds the methods we described above.
Intracanal anesthesia
Most often, this type of anesthesia is used already during treatment: for example, after infiltration anesthesia, the doctor, having started the treatment, understands that the patient has unpleasant and painful sensations and it is the addition of an anesthetic into the deep carious cavity or the opened mouth of the tooth canals that helps will soon continue work in a comfortable environment for the patient.
Also, the removal of painful teeth, accompanied by dividing it into parts, often requires the addition of anesthesia just inside the canals for painless extraction.
On the topic of general anesthesia, our wonderful doctors, anesthesiologists and resuscitators, have written articles that answer all questions and explain all the details of this topic. Of course, sleep treatment is used strictly according to indications, which include:
- treatment of children, which cannot be carried out in consciousness for various reasons,
- extensive surgical procedures of high complexity are also recommended to be carried out in a state of medicated sleep,
- the patient has intolerance to local anesthetics,
- psychosomatic and mental disorders.
In our clinic, this type of pain relief is provided by a team of anesthesiologist, resuscitator, intensive care nurse and, accordingly, a dentist and his assistant. Before treatment, the doctor collects anamnesis, the patient takes the necessary blood tests, etc.
To summarize, we can say that the fear of pain, which often holds us back from going to the doctor, should certainly have evaporated.
Modern drugs and techniques will not hurt you, doctors work in conditions that are comfortable for you, you can see and feel
We don’t want your pain at all: after all, this reduces productivity significantly! Your health comes first for us!
When is torsal anesthesia performed?
Torusal anesthesia is used for complex dental pathologies, when there is a need to anesthetize a large volume of tissue of the lower jaw:
- Therapeutic treatment of dental caries with severe pain syndrome;
- Extraction of mandibular teeth;
- Use of fixing splints for traumatic damage to the lower jaw;
- Extraction of teeth whose growth and formation are impaired;
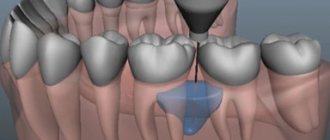
- Interventions to remove cystic cavities and neoplasms of the lower jaw;
- Difficulties in removing a mandibular tooth that for some reason is stuck in the bone;
- Opening of purulent cavities (thorusal anesthesia in combination with other methods of eliminating sensitivity);
- The eruption of a wisdom tooth through a dense area of gum with mucous membrane, which is swollen, inflamed, very painful and has a risk of rupture.
A contraindication to this type of anesthesia may be a violation of the anatomical integrity of the junction of the nerves, congenital defects of the lower jaw, gums, which will prevent the correct movement of the needle.
Why is torsal anesthesia dangerous?
If medical errors were made during pain management, the following negative consequences may occur:
- loss of nerve sensitivity of the mucous membrane of the throat;
- injury to the internal pterygoid muscles;
- trauma to blood vessels, leading to bleeding and hematomas;
- entry of the anesthetic into the bloodstream, which leads to ischemia of the skin of the lower lip and chin;
- convulsions and partial paralysis of facial muscles;
- nervous system disorders;
- needle fracture, requiring surgery to remove it;
- development of post-injection inflammation when infection occurs during an injection.
When performing an anesthetic injection, movements must be careful, smooth and precise, the instrument must be of high quality and sterile. Then the risk of undesirable consequences will be minimal. In addition, the patient must maintain full oral hygiene after the injection.
In some patients, torsal anesthesia can cause an unpleasant taste in the mouth, a burning sensation in the oral mucosa, and pain.
Regardless of the technique used, pain relief has a negative effect on the liver. Therefore, it is advisable for the patient to take medications after the procedure to promote its recovery.
When torusal anesthesia is contraindicated
This method of pain relief, like any mandibular anesthesia, is contraindicated in liver pathologies, since all anesthetics except novocaine create excessive stress on the liver. If you need to carry out a complex and lengthy operation on a large area of the jaw, then in this case, for the desired effect, a dose of novocaine will be required that is too large, exceeding the permissible limit. Therefore, local anesthesia is not used in such situations.
Contraindications to torusal anesthesia are also:
- allergy to local anesthetics;
- epilepsy;
- mental pathologies;
- cardiovascular pathologies;
- bronchial asthma;
- blood diseases.
During pregnancy, the permissibility of using anesthetics is determined by the level of possible danger to the fetus. In a separate article, we described in detail all the moments when teeth cannot be treated with anesthesia during pregnancy.
In general, the question of how acceptable local anesthesia is is decided for each patient individually, based on all the nuances of his health condition.