4990
One of the serious pathologies of the oral cavity structure that needs correction is the shallow depth of the vestibule.
It is impossible to manage with therapeutic measures in this situation, so the patient will have to undergo a surgical procedure - vestibuloplasty.
The technique will help not only restore the aesthetic appearance of the oral cavity, but also reduce the risk of developing severe complications.
Symptoms
The vestibule of the oral cavity is a gap of soft tissue that is located between the lip or cheeks and the elements of the dentition.
A variant of the norm is the depth of the vestibule from 5 to 10 mm. If this indicator does not reach 5 mm when measured from the end of the gum to the stationary area of the mucous membrane, dentists diagnose a shallow vestibule of the oral cavity.
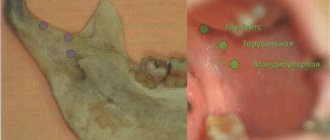
An anomaly in the size of the vestibule can be identified by the following signs:
- excessive narrowing or complete absence of the attachment zone of the mucous membrane;
- tension of the gum tissue in the area of the periodontal junction;
- inflammation and bleeding of the gums;
- increased sensitivity of incisors;
- exposure of the necks and roots of bone organs in the area of attachment of ligaments;
- dentofacial deformities;
- the presence of a short frenulum;
- violation of diction.
With a decrease in the size of the upper vestibule, incomplete closure of the lips, their partial immobility, as well as malocclusion and a reduced size of the upper jaw compared to the lower jaw may be observed.
Plastic surgery of tongue and lip frenulum
In addition to vestibuloplasty, plastic surgery of the frenulum of the tongue and lips is often performed in dentistry.
The pathological condition of the frenulum can lead to many problems and inconveniences, such as:
- problems with diction,
- interference with normal food intake,
- gap between the front incisors,
- gum recession,
- periodontitis,
- malocclusion.
- In infants there is a dysfunction of sucking.
During plastic surgery of the frenulum of the tongue, the latter is dissected, then the lateral edges of the mucous membrane are compared using transverse sutures to capture deep-lying tissues. Labial frenuloplasty is performed by making an incision around the frenulum, then the fibers are separated and displaced from the bone, after which sutures are placed
Causes
A small vestibule of the oral cavity can be the result of both surgical intervention and congenital pathology.
Acquired pathology is a consequence of the following points:
- surgery to correct nonunion of the upper lip;
- surgical interventions to eliminate the consequences of burns, mechanical trauma to soft tissues, and removal of tumors.
The cause of a congenital reduction in the size of the vestibule is most often heredity and the presence of certain pathologies in the development of the dentofacial apparatus.
What is a crooked jaw and methods for straightening it.
We will tell you here about how long the swelling lasts after compactosteotomy.
At this address https://orto-info.ru/zubocheliustnye-anomalii/zubov/polozheniya/etiologiya-razvitiya-i-metodyi-korrektsii-protruzii.html we will discuss why tooth protrusion occurs after braces.
Prognosis of vestibular bone plate augmentation in complex orthodontic treatment
The principles of traditional orthodontic treatment are based on taking into account the initially available volume of bone tissue, but if the range of tooth movement exceeds the boundaries of the alveolus, the risk of complications in the form of recessions increases. The odds ratio for developing recession in adolescent patients undergoing orthodontic treatment is almost 4.48 times higher than in patients who have never undergone orthodontic interventions. Essentially, the problem of recession during orthodontic treatment is caused by insufficient bone volume relative to the need to adapt the proper position of the tooth. Crowding of teeth in conditions of deficient jaw size provokes a vestibular inclination of units of the dentition, which, in turn, compromises the condition of the vestibular bone plate, the level of blood supply and periodontal status.
The mandibular incisors are the most susceptible to the risk of complications during orthodontic treatment. To prevent such disorders, as well as to optimize the outcome of orthodontic interventions, it is recommended to use a combined surgical-orthodontic approach. The technique of orthodontic-surgical interventions was first developed by Wilcko, and since then many modifications have been proposed, which involved performing controlled surgical trauma in order to activate the process of tooth movement. These approaches involve the surgical phase of treatment in the form of pre-orthodontic surgical periodontal augmentation, piezo incision, and accelerated periodontal intervention. In addition to speeding up the treatment process, it is also possible to increase the volume of bone tissue within which it is possible to move teeth. Thus, surgically optimized orthodontic treatment (COOL) is aimed at performing two tasks: improving and increasing the biotype of periodontal tissue (both soft and hard), and also accelerating the process of tooth movement by implementing the phenomenon of local acceleration. Despite the fact that modification of the biotype of periodontal tissues is the primary goal of COOL, before carrying out such manipulations it is necessary to take into account a number of anatomical limitations and the influence of etiological factors associated with the thin biotype of tissues and impaired blood supply. Historically, the term "regeneration" was used in cases of augmentation procedures around teeth, and implied reformation of the periodontal ligament, bone tissue and cementum. In this article, however, the authors will use the term “generation” instead of “regeneration” to describe the process of formation of alveolar bone tissue in areas where it was initially absent or too thin.
The purpose of this article is to review the various factors that can potentially influence the prognosis of buccal bone plate formation during the COOL procedure. In addition, in this article we will also discuss possible modifications in the COOL protocol to achieve the most effective results of the intervention. Based on the experience of the authors, all factors that could potentially influence the final result of regenerative interventions during orthodontic treatment can be divided into three main categories: those associated with the patient, those associated with the orthodontic treatment itself, and those associated with the surgical phase of the intervention and the material. , selected for augmentation. In this article, we will pay more attention to patient-related factors and factors related directly to orthodontic treatment, while factors related to the surgical phase of treatment and the choice of augmentation material will be discussed in our subsequent publications.
Patient-associated factors
There are many factors associated with the specific anatomy and morphology of the maxillofacial and dentoalveolar components, which not only affect the geometric dimensions of the alveolar bone tissue, but can significantly compromise the final result of rehabilitation if their significance is ignored during complex treatment. Vertical facial pattern has been identified as a determinant of alveolar morphology of the mandibular symphysis and the position of the lower incisors at class 1 and class 3 relationships. In addition, it was noted that patients with a short face type and class 3 ratios are characterized by a greater width of alveolar bone tissue. At the same time, in patients with normal facial length and a long face type with class 3 relationships, there is physiological compensation of the morphology of the symphysis due to lengthening, which significantly affects the position of the incisors. This form of compensation is associated not only with the thinning of the alveolar bone tissue, but also with the shape and position of the chin (photo 1-6).
Photo 1. Pronounced structure of the symphysis, visualized on the cephalogram.
Photo 2. Visualization of the volume of the bone graft, taking into account the potential level of its shrinkage necessary for the implementation of COOL.
Photo 3. View after suturing. Pay attention to the sufficient volume of the vestibule of the oral cavity.
Photo 4. Visualization of slight discolouration of the flap in the postoperative period.
Photo 5. CBCT sections before the onset of COOL. The presence of initial digescence on the vestibular side of the anterior teeth of the lower jaw.
Photo 6. CBCT sections after COOL. A compromise result of regenerative treatment, which is obviously associated with the presence of initial digiscence, the influence of the presence of a pronounced structure of the symphysis and tension from the muscles in the chin area.
Previous publications have already described the phenomenon of the influence of muscle pressure on the process of bone tissue resorption, which was especially pronounced after the completion of jaw growth. Patients who underwent forward-upward genioplasty, which consequently resulted in muscle release, were characterized by an increase in bone thickness over the symphysis region. There is also a specific relationship between the inclination of the lower incisors and the morphology of the alveolar bone tissue. For example, with lower incisors inclined forward and compensated class 2 relationships, a rather thin vestibular bone plate is noted. Under such conditions, vertical orthodontic movement of teeth can provoke iatrogenic damage to bone tissue, which will reduce the predictability of orthodontic manipulations as such.
Periodontal biotype
Analysis of CBCT sections obtained during the study of cadaveric material confirmed the presence of a relationship between the biotype of the gums and the thickness of the buccal bone plate. The need to take into account the biotype when implementing COOL is justified by the role of blood supply to the bone and soft tissue structures of the periodontium (photo 7-9).
Photo 7. CBCT sections before the onset of COOL. Deficiency of trabecular bone tissue in the frontal areas of the lower jaw, which also indicates a deficiency of blood supply.
Photo 8. CBCT sections 11 months after treatment. Visualization of minimal additional bone volume.
Photo 9. Visualization of the intervention area during surgery. The deficiency of bone blood supply suggested by the CBCT results was also confirmed clinically by the absence of significant bleeding after the corticotomy procedure.
The blood supply to bone tissue is directly related to the bone thickness parameter and directly affects the final result of treatment. As for the blood supply to the gums, it is provided both by the main vessels of the supraperiosteal region and by the vessels of the alveolar process. Thus, if the blood supply to the gums is deficient due to the thin structure of the bone tissue, then under such conditions not only the risk of recession increases, but also the risk of complications associated with pathological healing of iatrogenic injury. Classic scientific publications indicate that the thicker the soft tissue flap, the more blood vessels it contains, therefore, the higher the predictability of the effectiveness of its use for covering areas of the exposed root surface. Based on this, the result of the formation of a bony vestibular plate through augmentation in a thin tissue biotype during COOL can be quite limited due to a lack of blood supply to the soft tissues. To prevent such complications, it is necessary to carry out a comprehensive reconstruction of periodontal tissue, which will avoid exposure of the installed graft.
Alveolar process thickness and tooth position
For the success of any regenerative manipulations, it is necessary to ensure sufficient cell migration, supply of nutrients and an adequate amount of oxygen. All this depends on the intensity of the blood supply, which, in turn, depends on the initial anatomy of the alveolar bone tissue. To assess this, it is necessary to analyze the results of CBCT scanning, which will verify the density and architecture of the trabecular and cortical components. Previously, several variants of classification of alveolar bone and bone dislocations have been proposed, which made it possible to associate them with the risk of developing recession during orthodontic tooth movement. The Richman and Evans classifications suggest that the presence of 1-2 mm of bone tissue thickness can sufficiently minimize the risk of developing such complications. One of the classifications involves the differentiation of bone tissue in the coronal and root areas of the tooth, taking into account its planned position, thus arguing for the need for augmentation of specific areas in order to maximize the postoperative volume of the bony vestibular plate. The same approach can be used to select certain clinical cases suitable for implementing the COOL algorithm. From a regeneration perspective, compact bone tissue has a more negative impact on the intensity of blood supply and the outcome of bone plate thickening compared to soft trabecular bone structure (Figure 7-8). It is extremely important to carefully approach the selection of cases for implementing the COOL protocol, based on the anatomy of the alveolar bone tissue to ensure maximum predictability of complex rehabilitation. According to the authors, in cases of the presence of a thin tissue biotype, modifications of the COOL approach provide for the possibility of using soft tissue augmentation with a minimally invasive surgical approach, and in some cases, proliferative agents such as fibrin enriched with platelets, or plasma derivatives enriched with growth factors that promote activation process of angiogenesis.
Depth of the vestibule of the oral cavity
The prevalence of complications in the soft tissue area during regenerative procedures ranges from 0% to 45% on average. Performing regenerative interventions involving coronal positioning and primary healing of the surgical site in the frontal region of the lower jaw is very difficult due to the influence of a number of anatomical factors (photos 10-13). These include the tension of the mental muscles, the depth of the vestibule of the oral cavity, which affects the possibility of primary wound healing, taking into account the influence of tension from the lip, and tissue thickness. If the vestibule depth is deficient or the chin muscles are excessively tense, there is an increased risk of developing soft tissue discolourations, flap opening, loss of biomaterial, infection, and exposure of bone material or the membrane/acellular dermal matrix used. In patients with a shallow oral vestibule, the recess can be manipulated using a free gum graft or Botox injection.
Photo 10. Shallow vestibule of the oral cavity: view before performing COOL.
Photo 11. Suturing after performing the COOL phase.
Photo 12. View 2 weeks after the intervention: dislocation of the flap due to tension caused by the factor of the small vestibule.
Photo 13. The final result after COOL: deficiency of attached gums while achieving normal teeth position.
Factors associated with orthodontic treatment
Factors associated with orthodontic treatment that influence the regenerative outcome of COOL are primarily related to the specific mechanics of tooth movement relative to the available volume of bone tissue. Preliminary literature suggests an increased risk of recession during orthodontic treatment. Most often this is due to orthodontic movement of teeth in conditions of bone tissue deficiency, or in conditions of a thin biotype of periodontal tissue. On the other hand, if orthodontic movement is carried out taking into account the above-mentioned parameters, then the final achieved position of the teeth, on the contrary, contributes to the stabilization of bone tissue. Evans et al have previously discussed the different types of biomechanics of orthodontic tooth movement based on tooth position and available bone volume. The researchers also developed a classification of the position of teeth before treatment, based on the criteria of which it is possible to predict the risk of developing certain complications. In order to minimize the risk of developing recessions, it is necessary to analyze CBCT sections of the dentoalveolar complex, which would include designing a process for changing the position of the tooth from the existing one to the desired one. Thus, it is possible to identify patients with risk factors even before the actual start of treatment, as well as to select the most appropriate orthodontic movement mechanism that would allow achieving a stable position of not only the tooth, but also the surrounding bone tissue in the final result. Animal studies have confirmed that there is no restriction of tooth movement by the augmentation material used. On the other hand, orthodontic tooth movement induces integration and remodeling of the established bone graft. We should also not forget about the phenomenon of regional acceleration. This phenomenon not only promotes faster tooth movement, but also faster bone metabolism. One of the main aspects of orthodontic treatment remains the time required to achieve the maximum level of bone biomaterial metabolism and the range of movement required. Literature data indicate that the use of orthodontic force induces remineralization of the bone matrix, in the structure of which teeth move and remodel the bone substitute. After corticotomy, demineralization of the alveolus around the tooth being moved develops, while the collagen matrix of the bone tissue moves along with the tooth. Therefore, it is extremely important to begin orthodontic treatment within 2 weeks after augmentation to maximize the regenerative potential of the regional acceleration phenomenon. Before surgery, it is also important to obtain information from the orthodontist regarding the required degree of tooth movement needed to correct existing malocclusions. The range of movement required will determine the amount of augmentation required to compensate for the potential risk of developing dehiscence.
conclusions
For over a decade, the COOL approach has been used to treat dental patients with crowded teeth and/or jawbone size discrepancies. However, before starting any orthodontic treatment, it is necessary to determine the etiology of the patient's existing gum recession. In addition, it is extremely important to assess the initial volume of bone tissue within the boundaries of which orthodontic movement will be carried out. If the range of required movement exceeds the existing bone boundaries of the socket, this can be regarded as one of the indications for the implementation of COOL. Before starting the augmentation phase, it is necessary to assess the presence/absence of a thin biotype of periodontal tissue and other factors associated with the development of recessions or digescences. Correcting these before surgery helps achieve a more predictable rehabilitation result. The physician must also understand the basic principles of the influence of muscle tension, the morphology of the mandibular symphysis and the small vestibule of the oral cavity on the possible outcome of treatment. Assessing the ratio of the required range of tooth movement to the available volume of bone tissue through analysis of CBCT slices is one of the most important stages in planning a COOL procedure. Another factor that guarantees successful treatment is the rehabilitation of the patient with the involvement of a multidisciplinary team of specialists, whose deep understanding of the situation will significantly increase the predictability of the surgical and orthodontic rehabilitation carried out.
Authors: Stuart Beauchamp, DMD Colin S. Richman, DMD William Baldock, DMD Brock J. Pumphrey, DMD J. Kobi Stern, DMD, MSc
Consequences
The depth of the vestibule and the attachment of the gums play an important role in the process of protecting the marginal periodontium from external influences.
In case of insufficient attachment or complete absence of attached gum tissue, the following problems may arise:
- trauma to the marginal periodontium while eating food;
- increased muscle tone of the chin;
- impaired blood supply to gum tissue;
- formation of pathological bite;
- partial decrease in lip mobility;
- slower growth of the upper jaw row;
- loosening of teeth;
- inflammatory diseases of the gums, their atrophy;
- development of periodontitis.
Indications for surgery
Vestibuloplasty is indicated in the following cases:
- absolute absence of gum attachment;
- a symptom of tension, the signs of which are pallor and displacement of the gingival margin when the lip is pulled back;
- lack of attached gum zone – distance less than 1 mm;
- signs of inflammation of the gum tissue;
- preparation for orthodontic therapy - installation of a structure to correct the bite will not bring the required effect with a small vestibule due to the fact that the alveolar processes of the incisors will return to their original position due to gingival tension;
- the need for further prosthetics;
- elimination of recession or atrophy of gum tissue.
The small vestibule of the oral cavity is often diagnosed not only in adults, but also in childhood. In this case, during the mixed dentition, observation of the child by the dentist is indicated. The operation is permissible after complete eruption of all teeth.
Course of action
Before proceeding with surgery, the dentist conducts a thorough examination of the patient’s oral cavity using certain instruments and equipment.
This allows you to identify associated problems and determine the most suitable vestibuloplasty technique among the many existing ones.
Before the operation, the dentist also professionally removes mineralized plaque from the front surface of the dentition.
During preparation for surgery, the patient is required to comply with the following rules:
- refusal to take painkillers and other medications not prescribed by the dentist;
- refraining for 6 hours before surgery from consuming foods that can cause mechanical injury to the gum tissue.
Vestibuloplasty is performed with preliminary anesthesia of the treated area. Anesthesia can be either local or general, at the request of the patient.
There are many options for performing surgery to change the size of the vestibule, which can be divided into several large groups.
Open method
Open vestibuloplasty techniques are based on changing the depth of the vestibule in such a way that a wound is formed on the surface of the lip and alveolar process, which takes about two weeks to heal.
The key disadvantage of such methods of surgical intervention is the formation of scars on the soft tissue, which in the future can contribute to the re-development of the pathology.
The open method is carried out as follows:
- a dissection of the mucous membrane of the lower lip is performed using an incision in the sector of the front teeth;
- an apron-shaped flap is peeled off, the base of which is a transitional fold in the area of the incisors;
- soft tissues are displaced to the prescribed depth, which helps to increase the depth of the vestibule;
- the detached flap of tissue is placed in the area of the alveolar process of the lower jaw, after which it is fixed with suture material;
- the wound formed on the mucous membrane is sutured and healed due to secondary intention.
Closed
Plastic surgery using a closed surgical technique involves closing the wound surface formed after enlargement of the vestibule using local soft tissue.
The essence of the method is that soft tissue is cut off through a small vertical incision.
The mucous membrane is practically not damaged. Thanks to this, the recovery process proceeds more quickly.
Dentists note a significant drawback that is inherent in closed operations - the possibility of relapse of the disease. According to statistics, three years after the operation, the size of the vestibule is again reduced by almost half.
Patchwork
The key indication for flapplasty is the exposure of the necks and roots of the teeth due to the strong tension of the soft tissue, which over time can lead to inflammation of the gum tissue and loosening of the teeth.
During vestibuloplasty, several horizontal and vertical incisions are made, which allow the edge of the gum tissue to be excised to form a flap.
After this, the separated flap is placed in the intended place in the dentition and fixed with suture materials.
Use of the plate
Vestibuloplasty using special plates is practically no different from the methods described above, however, its peculiarity is the use of a forming plate during the final stage.
This vestibular structure is applied to the wound surface after applying the flap and fixing it with sutures. The duration of its use is about two months.
Possible causes of crowded teeth in the lower jaw and ways to eliminate the anomaly.
In this publication we will talk about the reasons for the development of a small lower jaw in a child.
Follow the link https://orto-info.ru/zubocheliustnye-anomalii/ryadov/zuboalveolyarnogo-ukorocheniya.html if you are interested in the operation of dentoalveolar shortening.
Using laser in vestibuloplasty
Laser vestibuloplasty is the most innovative and gentlest procedure. The use of this technology allows you to clearly plan and organize the operation. The advantages of this method include:
- fast recovery;
- minimal damage to nerve endings;
- the ability to make a precise cut without bleeding;
- allows you to avoid tooth enamel sensitivity and tissue burns;
- eliminates the risk of infection;
- improves the fit of contacting tissues;
- prevents the development of the inflammatory process;
- has a stimulating effect on the process of tissue restoration;
- does not lead to scarring.
The medical center provides treatment for all types of dental diseases. You can make an appointment with a doctor on the website of this clinic. At the appointment, the doctor will conduct an examination, diagnosis and give advice on further treatment of the identified pathologies.
Other treatments
Among the above methods, there are some variations, the choice of a specific one is made by the dentist after examining the patient’s oral cavity.
Edlan-Meicher method
This method is most often used when it is necessary to eliminate a small vestibule on the lower jaw due to its high efficiency.
After anesthesia of the operated area, an incision is made into the mucous membrane along the bend of the bone arch. Next, the mucous membrane and periosteum are peeled off, as well as the submucosal tissue moves to the lateral and anterior sections of the vestibule.
For fixation, sutures are placed on the mucous membrane, after which the wound is covered with a special bandage. The patient's recovery time is about two weeks.
The performance of vestibuloplasty according to Meyhar can be seen in the video.
Schmidt method
The Schmidt technique differs from the previous version of the operation only in that exfoliation of the periosteum tissue is not performed.
The soft and muscle tissues in this sector are also incised along the periosteum. The resulting flap edge is placed deep into the formed vestibule and then fixed.
This method of vestibuloplasty is equally effective for treating both the lower and upper jaw.
Glickman method
Plastic surgery using the Glickman method can be performed both on a limited sector of the oral cavity and on a larger area.
After administering anesthesia, the surgeon dissects the mucous membrane in the area of its attachment to the lip, then detaches the soft tissue and forms a depression.
After this, the detached section of the mucous membrane is attached to the resulting depression.
Clark's method
Plastic surgery of the small vestibule using the Clark method is performed for pathology of the upper jaw row.
After administering the anesthetic drug, a section is made at the border of the junction of the gingival margin and the moving section of the mucous tissue of the vestibule.
Using scissors, the mucous surface of the upper lip is peeled off. The soft tissue of the vestibule is dissected as close as possible to the periosteum and parallel to the curvature of the bone surface. The depth of the cut should not exceed 15 mm.
The previously detached section of the mucous membrane of the lip is placed in the vestibule formed as a result of tissue dissection, and then secured with sutures.
At the end of the procedure, the wound is covered with an iodoform swab.
Tunnel vestibuloplasty
The least traumatic method of plastic surgery, which is used to correct the depth of the vestibule of both jaws, is tunnel vestibuloplasty.
In certain areas of the oral cavity, two horizontal incisions are made along the premolars, as well as one vertical in parallel with the frenulum. After this, the mucosal flap is shifted inside the formed vestibule and secured.
The wound surface during this procedure is significantly reduced compared to other surgical techniques. The duration of the rehabilitation period practically does not exceed 10 days.
Technique of vestibuloplasty
Depending on the cause of the defect and the purpose of vestibuloplasty, the operation can be performed using different methods:
- According to Clark. This option is considered optimal for correcting the upper jaw. In this case, the periosteal tissue is not affected even if a large area is dissected. The incision is made along the transitional fold located between the gum and mucous tissue. The healing period is 15-20 days.
- Tunnel operation. It is closed and minimally traumatic. Used to correct both the upper and lower jaws. 3 small vertical incisions are made along the frenulum and 2 horizontal incisions along the connective tissue towards the premolars. Thus, manipulations are carried out with the mucous membrane. It takes 9-12 days to heal.
- According to Elan-Meicher. Mainly suitable for correction of the lower jaw mucosa. The incision is made parallel to the curve of the jaw. It takes about 14 days to heal.
- According to Glickman. The method is used for local areas of different areas. The lip attachment site is incised to 15 mm in depth. After which the mucous membrane is displaced and sutured.
- According to Schmidt. During the operation, only the mucous membrane is affected. After manipulation using this method, a pressure bandage is applied to the chin and a shaping bandage is applied to the teeth.
- According to Limberg. The dissection is carried out along the frenulum to form two triangular flaps. After separating the mucous tissue, the flaps are crossed and sutured.
Rehabilitation
The duration and severity of the rehabilitation process depends not only on the dentist’s manipulations, but also on the patient’s compliance with the following recommendations:
- at the end of the procedure, use a cold compress to relieve swelling from the operated area;
- Avoid eating too hard, spicy or hot foods for two weeks after surgery;
- reduce the amount of dairy products consumed, as they contribute to the formation of persistent plaque;
- use soft-bristled toothbrushes for daily hygiene;
- rinse the mouth with special anti-inflammatory and antiseptic drugs;
- after five days after the operation, begin performing myogymnastic exercises recommended by a specialist;
- visit the dentist on the appointed days to monitor the recovery process.
Stages of dental examination
The patient undergoes examination in three stages.
- clarification of complaints and medical history;
- examination using physical methods (inspection, palpation, percussion, auscultation);
- research using special methods (laboratory, x-ray).
The final clinical diagnosis is made after clarifying complaints and other aspects of the disease and collecting additional information about the patient. All this will allow appropriate treatment to be carried out at the next stage.