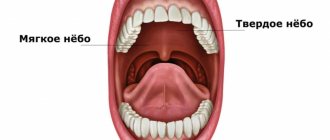
The palate is the upper wall of the mouth, divided into the hard palate, which forms the anterior two-thirds, and the soft palate, which forms the posterior third. The hard palate is formed in the anterior section by the palatine processes of the maxillary bones, in the posterior section by horizontal plates of the palatine bones. The soft palate is a fold of mucous membrane that contains connective tissue and muscles. Cells of the mucous membrane covering both parts of the palate can become a source of malignant neoplasm - palate cancer.
In essence, palate cancer is a special case of cancer of the oral mucosa. Cancer of the hard palate accounts for 4% of all tumors in this location, cancer of the soft palate - 6.2%. Since the hard and soft palates are represented by different tissues, the histological subtypes of detected cancers also differ: squamous cell carcinoma most often develops from the structures of the soft palate, cylindroma (adenocystic cancer), adenocarcinoma, and less often squamous cell carcinoma develops from the hard palate.
In addition, a tumor of the palate may not be an independent disease, but a metastasis of another cancer located in the head and neck area.
Risk factors
Among the main factors predisposing to the development of palate cancer are the following:
- bad habits: smoking, especially in combination with drinking strong alcohol, chewing various mixtures (for example, betel);
- precancerous conditions that can develop into a malignant tumor,
- chronic inflammation of the oral mucosa;
- factors of chronic mechanical trauma to the oral mucosa (destroyed teeth and their roots, poorly manufactured dentures);
- work in hazardous industries (contact with carcinogens, work in high temperatures);
- lack of vitamin A;
- eating too hot and too spicy food.
Separately, I would like to dwell on diseases that are obligate, that is, with a high frequency of malignancy, and facultative, with a low frequency of malignancy, precancerous conditions.
An obligate condition for palate cancer is Bowen's disease - single or multiple neoplasms of the mucosa, localized in its surface layer. In the early stages of its development, the neoplasm looks like a reddish spot with jagged edges. The spots grow slowly, and when several spots are located close to each other, they can merge. With further growth, the spots may peel off, and depressions or growths may appear on them.
Throughout its progression, Bowen's disease does not manifest itself as pain or itching. The degeneration of Bowen's disease into cancer is indicated by the appearance of ulcers on the plaque.
Bowen's disease is often considered a cancer in situ and requires immediate surgical treatment when diagnosed.
Optional precancerous diseases include:
- Leukoplakia - flat, whitish areas of the mucous membrane, smooth to the touch and with a soft consistency. Flat leukoplakias may remain unchanged for many months, without thickening or ulcerating. The incidence of cancer due to leukoplakia varies according to different authors and ranges from 15-75%.
- Erythroplakia is a red area of the mucous membrane raised above the surface, which is easily injured and bleeds. In 70% of cases it leads to the development of cancer (and according to a number of authors, with long-term existence of erythroplakia, this probability increases to 80-100%).
- Leukokeratosis is the proliferation of squamous epithelium. Upon examination, it looks like whitish spots of various shapes, slightly rising above the mucous membrane of the soft palate. When palpating the area of leukokeratosis, a dense consistency and rough surface are determined.
- Papillomatosis is a papillary growth of connective tissue caused by infection with the human papillomavirus. In most cases, papillomas develop against the background of progression of leukokeratosis.
Due to the risk of malignancy of the above formations, surgical treatment is necessary - either conventional excision of the affected areas of the mucosa, or cryodestruction or electrocoagulation can be performed.
Phases of development
Neoplasms, even of benign origin, after some time degenerate into a malignant tumor, which, as it progresses, goes through three stages of development:
- The initial form is characterized by unusual phenomena for the patient in the form of pain, ulcers, and lumps in the oral cavity.
- A developed form of the disease - the ulcers take on the appearance of cracks, pain appears, radiating from the mouth to different parts of the head. There are cases when the patient does not feel pain at this stage.
- An advanced form is the active phase of cancer, when lesions spread quickly. Associated symptoms are also noted: pain in the mouth, difficulty swallowing food, a sharp decrease in body weight, and a change in voice.
Symptoms of palate cancer
At the very beginning of the development of the disease, as with many other types of cancer, there may be no complaints. At this stage, identification of a lesion in the palate may be an incidental finding during examination by a dentist or otolaryngologist. The main complaint with which patients consult a doctor in the initial stages of cancer is discomfort during eating in the form of burning or tingling. When the tumor is localized in the mucous membrane of the soft palate, a “sore throat” may also occur, which can be mistakenly recognized as a consequence of the inflammatory process.
Against the background of one of the precancerous processes described above or on the unchanged mucous membrane of the palate, a small compaction or papillary growth, a flat or slit-like ulcer with a ridge-like edge and a compacted bottom (the most common variant, detected in approximately 50% of cases), white spots appear.
Conservative treatment may be prescribed for detected tumors. It is important to remember that in a situation where the possible causes of the formation of an ulcer or fissure have been eliminated, but the treatment carried out after 10–15 days has been unsuccessful, a diagnosis should be made for the presence of a malignant formation.
As the size of the neoplasm increases, its pressure on the mucous membrane increases, and an area of ulceration may appear or increase in size, which, in turn, may become infected. Taken together, this leads to the appearance of pain. The pain can have varying intensity, be local in nature, or radiate to one or another area of the head, most often to the ear and temporal region on the affected side.
In many patients, salivation increases as a result of irritation of the mucous membrane. If the tumor begins to disintegrate or an infection develops, foul breath appears.
In the case of a severely advanced process, palate cancer destroys the surrounding tissues - bones, muscles, other structures that form the oral cavity, skin, which determines the appearance of new symptoms. In addition to severe pain, speech and swallowing disorders develop, which leads to exhaustion. In case of tumor damage to the muscles, it becomes difficult to open and close the mouth. If the tumor disintegrates, bleeding develops, which is difficult to control and can be life-threatening. Finally, pneumonia may occur, which can lead to the death of the patient.
Complications
Palate cancer is a dangerous disease. The head and neck are supplied with blood extremely well, so all pathological processes spread in the shortest possible time. Nearby are vital organs - the brain, respiratory tract, large blood vessels (branches of the external and internal carotid arteries), and nerve trunks. When these structures are involved, the prognosis becomes unfavorable.
Once the tumor ulcerates, there is a high risk of secondary infection and microorganisms entering the blood. In conditions of reduced immunity, a septic condition will occur, characterized by multiple organ failure.
When cancer grows into blood vessels, life-threatening massive bleeding is possible. An increase in the size of the tumor threatens to form a mechanical obstruction to the passage of air into the lungs, in which case asphyxia will develop.
Diagnosis of palate cancer
Diagnosis begins with a medical history with mandatory identification of risk factors for cancer and a physical examination. The tumor is characterized by three forms of growth:
- exophytic, in which mushroom-shaped or plaque-like growths are detected on the mucous membrane with clear boundaries;
- endophytic (ulcerative, infiltrative or ulcerative-infiltrative)
- mixed.
To verify the diagnosis of cancer, a biopsy of the palate formation is necessary. A biopsy can be performed in several ways:
- Brush biopsy is a relatively new method, the advantage of which is that it is painless; therefore, it does not even require local anesthesia. Material from the surface of the tumor is taken using a special brush and further examined. If the material is not informative enough, a standard incisional biopsy is subsequently performed.
- Incisional biopsy is the most common and most informative method. In this case, the formation suspicious for cancer is excised completely under local anesthesia (less often, under general anesthesia, in the case of a difficult-to-reach location of the formation), and the entire tumor is sent for histological examination.
- Fine-needle aspiration biopsy - with this method, material is collected for histological examination by puncture of the formation with a thin needle.
To clarify the diagnosis, an additional immunohistochemical study may be prescribed.
To assess the prevalence of cancer, the following instrumental diagnostic methods are prescribed:
- ultrasound examination of the lymph nodes of the neck and oral tissues,
- computed tomography or magnetic resonance imaging of the affected area,
- ultrasound examination or computed tomography of the abdominal cavity and retroperitoneal space,
- X-ray or computed tomography of the chest,
- Positron emission tomography may be prescribed, especially in cases of recurrent tumors and significant spread of cancer.
In addition, an analysis for the presence of papillomaviruses may be prescribed. Up to 70% of patients with oral cancer of various locations, including palate cancer, are carriers of papillomaviruses. Infection with papillomavirus type 16, less commonly type 18, which have a high risk of oncogenicity, may be one of the factors leading to the development of cancer of the soft palate.
Forecast
Completely overcoming the disease is only possible with early diagnosis and the correct choice of treatment method.
The prognosis is that it is possible to completely overcome the disease only with early diagnosis and the correct choice of treatment method.
The result also depends on the type of cancer.
For example, the papillary variety is much easier to cure. The most difficult thing is with an ulcerative neoplasm.
The relapse-free period (up to 5 years) after a course of isolated therapy is 70-85%; with the development of a tumor on the floor of the mouth, the figure is lower (46-66%).
When diagnosing stage 3 oral cancer, according to statistics, the absence of relapses is observed in 15-25%.
Stages of palate cancer
Palate cancer is staged according to principles common to most malignant tumors - according to the TNM system, which involves assessing the size and extent of the primary tumor, the involvement of regional lymph nodes and the presence of distant metastases, and according to these parameters the following stages are distinguished:
- Stage 0 - cancer in situ. Only the superficial layers of the mucous membrane are affected without spreading to the underlying layers.
- Stage I - tumor up to 2 cm in greatest dimension, without damage to regional lymph nodes and distant metastases.
- Stage II - tumor from 2 to 4 cm in greatest dimension, without involvement of regional lymph nodes and isolated metastases.
- Stage III - a tumor more than 4 cm in greatest dimension, or a tumor node up to 4 cm with a metastasis less than 3 cm in size in one regional lymph node on the affected side.
- Stage IV - tumor spreading to nearby structures (for example, cortical bone, masticatory apparatus, pterygoid processes of the main bone or skull base); or metastases larger than 3 cm in size and/or in several lymph nodes, both on one side of the neck and on both; or the presence of distant metastases.
Treatment of palate cancer
Palate cancer is a chemo- and radiosensitive tumor, so these cancer treatment methods are widely used along with surgery. Treatment tactics are determined by the size of the tumor and the degree of involvement of regional lymph nodes. Thus, surgical treatment is not recommended for stage T4b, when there is significant invasion of surrounding bone structures, direct spread of the tumor from regional lymph nodes to the skin, spread to mediastinal structures or cervical vertebrae due to the unresectable nature of the process, intra- and postoperative risks, low efficiency and low probability of radical surgical treatment.
There are several options for surgical access, each of which has its own indications and contraindications. For tumors located closer to the vestibule of the oral cavity, it is permissible to use a transoral approach, for tumors of “posterior localization” - a median mandibulotomy. During surgery, the tumor is removed en bloc within healthy tissue. With a significant depth of invasion, it is possible to remove a large part of the palate. In this case, it is possible to use reconstructive plastic techniques using local flaps (mucoperiosteal flap), free flaps (for example, a musculocutaneous flap including the pectoralis major muscle, trapezius muscle), a split skin flap to cover the defect. A separate access is used to remove neck lymph nodes.
Treatment tactics vary depending on which part of the palate—hard or soft—is affected. So, when treating patients with hard palate cancer, the algorithm is as follows:
- In the first and second stages of the disease, removal of the primary lesion and prophylactic removal of regional lymph nodes are indicated. NCCN guidelines include the option of sentinel lymph node biopsy, but this technique is not currently widely used. If, according to postoperative histological examination, metastases in the lymph nodes or unfavorable prognosis factors are identified, chemotherapy or radiation therapy is carried out in the postoperative period. In some cases, when the patient refuses surgery or is inoperable due to concomitant diseases, a radical course of radiation therapy may be performed.
- In the third stage of the disease, when metastases in the lymph node have already been identified, cervical lymph node dissection is performed necessarily and more widely than in the prophylactic version. In the presence of bilateral lesions or lesions of the lymph nodes on the opposite side, lymph node dissection is performed on both sides. After surgery, in the presence of unfavorable prognosis factors, radiation therapy or chemotherapy, or a combination of both, is indicated.
If the soft palate is damaged, the treatment tactics are as follows:
- In the early stages of cancer, surgical treatment is performed, including bilateral lymphadenectomy. If unfavorable prognosis factors are identified in the postoperative period, radiation or chemotherapy is performed.
- At stage N1, when only one regional lymph node is affected, simultaneous chemoradiotherapy is performed.
- In the third or fourth stage of the disease, if technically possible, surgical treatment is performed followed by radiation therapy. Alternative options include chemoradiotherapy or two courses of induction chemotherapy followed by chemoradiotherapy.
If distant metastases are detected, the patient is prescribed chemotherapy. It is important to note that the presence of distant metastases is not a contraindication to surgery or radiation therapy to the area of the primary tumor - such tactics are acceptable if the number of metastases is small and the patient’s objective condition is good (Karnofsky index 90–100%).
Radiation therapy is administered to the area of the primary tumor and the lymph nodes of the neck on both sides. If treatment is carried out according to a radical program, then a single dose is 2 Gy, the total dose is up to 70 Gy for the tumor node itself and metastatically affected lymph nodes, for unaffected lymph nodes - up to 50 Gy.
Postoperative radiation therapy should be started no more than 3 months from the date of surgery, and the optimal period is 6 weeks, but it can only be started after complete healing of postoperative wounds. In this case, a smaller total dose is delivered to the bed of the removed tumor and the area of metastatically affected lymph nodes - 60–66 Gy, depending on the involvement of the resection edges in the tumor process; 50 Gy is also delivered to the intact lymphatic collectors.
In some situations, in addition to external beam radiation therapy, and also as an alternative, interstitial brachytherapy can be used. With low-dose brachytherapy, it can be performed in several sessions up to 60-70 Gy without external beam radiation and up to 20-35 Gy with another 50 Gy added at the stage of external beam radiation therapy; with high-dose - as a boost up to 21 Gy in 7 sessions after 40-50 Gy from external beam radiation therapy or up to 45-60 Gy with a single dose of 3-6 Gy in an independent version.
The following are used as chemotherapeutic agents:
- Cisplatin - if the patient is indicated for chemoradiotherapy, cisplatin is administered once every three weeks (on days 1, 22 and 43 of radiation treatment);
- Carboplatin - as an alternative to cisplatin to avoid nephrotoxicity;
- 5-fluorouracil - used in combination with cisplatin or carboplatin;
- Cetuximab - in the presence of concomitant pathology (in fact, contraindications to the use of platinum-based chemotherapy, for example, renal failure).
Induction chemotherapy involves the use of three-component regimens that include docetaxel or paclitaxel, cisplatin and fluorouracil.
I would like to separately note the possibility of cryodestruction of the tumor. Although this approach is not currently considered standard, it can be successfully used for the first stage of soft palate cancer in combination with radiation or chemoradiation therapy, provided the tumor responds to conservative treatment, as well as for localized recurrent tumors if surgical intervention is not possible. The undoubted advantage of this method is its low invasiveness for surrounding tissues, but it can be used in a small number of carefully selected patients.
Classification of oncological pathology of the palate
Depending on the location of the tumor, two types are distinguished: cancer of the hard palate, in which the pathological process affects bone structures; and cancer of the soft palate, affecting the mucous and muscular part of the vault. The cancerous growth appears as either a nodule or an ulceration.
Another classification is based on the source of tumor growth:
- Cylinder. The source of atypical cells is glandular tissue. This histological type of tumor is characterized by intensive growth and rapid formation of metastases.
- Adenocarcinoma. The tumor is of epithelial origin. It can occur with cancer of any part of the palate.
- Squamous cell carcinoma. It occurs in practice more often than other types. Cancer cells form in mucous tissue.
Medical professionals use the TNM classification. T (tumor) – characterizes the degree of damage to organ tissue by a tumor. It is divided into subtypes Tis, T1-T4, where Tis is pre-invasive cancer.
- T1 – the size of the tumor does not exceed two centimeters.
- T2 is a formation measuring two to four centimeters.
- T3 – stage with a tumor larger than four centimeters.
- T4 – cancer grows into nearby tissues.
Palate cancer
N (nodus) reflects damage to the lymph nodes. Classified by degrees from N0 to N3, when the lymph nodes are not affected, affected on one side, on both sides and fused with surrounding tissues, respectively.
The last characteristic is the presence of metastases, M (metastasis). Grade M0 is allocated when there are no metastases, and grade M if metastatic lesions are detected.
Treatment of recurrent palate cancer
Palate cancer, like any other malignant neoplasm, is capable of recurrence. Treatment of relapse is a significant challenge, since treatment performed on the primary tumor significantly narrows therapeutic options. Currently, in case of locoregional relapse, a second operation is performed, which should be aimed at achieving clean resection margins and further radiation or chemoradiotherapy, if it was not performed for the primary tumor; As an alternative, if surgery is not possible, chemoradiation therapy may be used.
If radiation therapy has already been carried out, then either surgery followed by chemotherapy or re-irradiation, possibly in combination with chemotherapy, is performed.
Types of tumor
A tumor on the roof of the mouth always indicates the onset of an inflammatory process in the human body. Tumors can be benign or malignant.
Malignant formation
Problems with the development of a malignant tumor are not limited to disturbances in speaking and eating. The lump, the cause of which is cancer, impairs articulation, complicates the ability to communicate or completely eliminates it.
Oral cancer is typical for men and is a local metastasis of other malignant tumors in the head. It is a rare cancer.
Such malignant lumps are classified as growths on the roof of the mouth. The tubercle can pop up due to a benign inflammatory process, so it is impossible to express a clear opinion about the diagnosis.
Understanding the reasons for the appearance of a tumor is important for determining the course of treatment. The causes can be accurately diagnosed by conducting clinical studies of the compaction.
Benign formation
A cyst on the roof of the mouth is not a fatal diagnosis; it is diagnosed with a number of benign tumors. Such tubercles are caused by insidious but curable diseases:
- growth of blood vessel tissue (angioma);
- cyst;
- pemphigus (erosion);
- myxoma.
Rehabilitation after treatment
Rehabilitation after treatment requires an integrated approach, which is based on lifestyle changes:
- Dieting. In the early postoperative period or after completion of radiation therapy, only liquid or puree foods are possible. As the tissues of the oral cavity heal, a transition to semi-solid and solid foods is possible. It is advisable to chew on the side opposite to the affected one.
- In case of nutritional deficiency, the patient may be prescribed intravenous or specialized therapeutic nutrition (for example, Nutridrink). Nutritional support is carried out in the presence of at least one of the specified factors: a decrease in body weight over the last 6 months by 10% or more, a decrease in protein levels in a biochemical blood test, a decrease in body mass index to a value of less than 20. These measures can be applied as before the planned surgery, as well as during chemotherapy and radiation therapy. In the postoperative period, nutritional support should be provided for 7 or more days.
- Drinking plenty of fluids is recommended. If patients with a palate tumor complain of dry mouth, salivary substitutes (eg, calcium phosphate solutions; gels containing lysozyme, lactoferrin, and peroxidase), salivary and taste stimulants (eg, xylitol chewing gum, sorbitol lozenges, or xylitol), pilocarpine may be used.
- Oral hygiene. Teeth brushing will be permissible after postoperative sutures have healed or radiation damage has resolved. In order to maintain hygiene of both teeth and mucous membranes of the oral cavity, it will be necessary to rinse or irrigate. Both soda solution or antiseptic solutions such as Miramistin, as well as special alcohol-free solutions are used. Rinsing should be done at least 4 times a day, including after each meal.
- Treatment of radiation damage. Radiation therapy, like any other treatment method, has its side effects, and due to the fact that a large total dose is delivered, they can be significant. During radiation therapy, as well as upon its completion, compliance with accompanying treatment measures is required: in addition to the above, the patient is prescribed ointment treatment of the skin of the irradiated area, after resolution of early radiation damage - applications with dimexide solutions of increasing concentrations in order to prevent the development of fibrosis. If significant damage to the mucous membranes develops, antibiotic therapy and antifungal drugs are prescribed to prevent infection.
- In the case of chemotherapy - either alone or in combination with radiation therapy - there may be a significant drop in blood counts, so careful and regular monitoring is necessary. It is possible to use hematopoiesis stimulants to prevent interruptions in treatment or the development of infectious complications.
- Restoration of speech function. If the operation was performed for cancer of the soft palate, then due to postoperative edema, speech may change. As the sutures heal, speech function will recover on its own, but in the case of extensive damage to the palate and the appropriate amount of surgical intervention, the help of a speech therapist may be required to restore speech.
- Swallowing. Surgery on the palate, especially the soft palate, can lead to swallowing problems. Both before the start of treatment and during its process, patients are prescribed special preventive gymnastics and training in swallowing tactics. In case of significant impairment of swallowing, the patient may have a nasogastric feeding tube installed.
- Therapeutic exercises can be prescribed to prevent lymphostasis in the area of surgery, as well as to prevent spasms of the masticatory muscles.
Prevention
The best prevention of palate cancer is early detection of both existing cancer and precancerous conditions. Therefore, to prevent cancer, periodic self-examination of the oral cavity and palate in particular is recommended. Regular, at least once a year, visits to the dentist for preventive purposes also play a big role in the early detection of diseases not only of the teeth, but also of the oral mucosa.
If precancerous conditions are detected, patients need clinical observation, especially if the diseases are difficult to treat or are prone to recurrence.
Since chronic inflammatory diseases can also cause the development of cancer, their treatment and regular sanitation of the oral cavity are required. Giving up bad habits - smoking and drinking alcoholic beverages - will have a positive effect. Finally, eating a nutritious diet, including plenty of vegetables and fruits several times a day and whole grain foods, will also help reduce your risk of cancer.
Patients who have already been diagnosed with palate cancer and have completed treatment also come under dispensary observation by an oncologist. In the first year, a control examination is carried out every 1-3 months, in the second year - every 2-6 months, for a period of 3-5 years - once every 4-8 months. After 5 years from the date of surgery, visits are carried out annually or when complaints arise. The frequency of visits is determined by the degree of risk of relapse. As part of the examination, an ultrasound scan of the lymph nodes of the neck on both sides and soft tissues of the oral cavity, abdominal organs, and, if necessary, CT/MRI of the head and neck area, and chest x-ray once a year are performed. If PET-CT was performed before the start of treatment, it is repeated no earlier than one year after completion of complex treatment.
Tumor lesions of the palate can be asymptomatic for quite a long time, which is why patients turn to the doctor with the process already quite advanced. However, modern treatment protocols make it possible to give hope for a cure for any stage of palate cancer. Euroonco doctors have all the necessary tools in their arsenal to provide treatment for palate diseases with the highest efficiency. Also, our specialists are always ready to advise you and your loved ones on precancerous conditions of the oral cavity and formulate a plan for further observation and treatment measures.
Book a consultation 24 hours a day
+7+7+78
Bibliography
- Malignant neoplasms of the oral cavity. Recommendations of the Association of Oncologists of Russia, 2021.
- Head and neck cancers. NCCN clinical practice guidelines in oncology, 2021.
- Tabolinovskaya T.D., Pustynsky I.N. Analysis of the effectiveness of cryogenic treatment of oropharyngeal cancer. Tumors of the head and neck. 2021, vol. 6, no. 2, pp. 56–59.
- Kropotov M.A. et al. Surgical aspects of treatment of recurrent oropharyngeal cancer. Malignant tumors. 2013. pp. 43–52.
- Lazarev A.F. Plastic component in the surgical treatment of patients with tumors of the oropharyngeal zone. Siberian journal of oncology. 2007, no. 1 (21). pp. 59–62.
Advantages of treatment in Israel
- The opportunity to be treated by world-class specialists at reasonable prices.
- Availability of modern diagnostic and treatment equipment in the clinic.
- Using the latest and most effective treatment protocols.
- Caring care during the stay for treatment and the services of a case manager, simplifying the patient’s stay in a foreign country.
- The ability to pay for services in any convenient form upon receipt of them.
If signs of the disease are detected in you or your loved ones, and you are interested in treatment in Israel, fill out the application form on our website or request a call back. Our consultant will contact you shortly and help organize your trip. There's no reason to put off applying, do it today!
- 5
- 4
- 3
- 2
- 1
(1 vote, average: 5 out of 5)