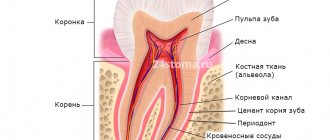
Anatomy of the trigeminal nerve
The trigeminal nerve (5th pair) is a large mixed (sensory-motor) nerve, consisting of three branches :
- Orbital (n. ophthalmicus).
- Maxillary (n. maxillaris).
- Mandibular (n. mandibularis).
The mandibular ( MF ) is the third branch of the trigeminal, innervating the skin, mucous membranes of the organs of the lower jaw, and the muscles of the lower part of the face. Its location and parameters in the human body are individual and determined by anatomical features. The nerve trunk consists of 30-80 fibers, thickness is in the range of 3.5-7.5 mm, length - 0.5-2.0 cm.
The roots of the mandibular nerve transmit information from the lower part of the face and oral cavity: teeth, gums, tongue, outer part of the ear. Motor - innervate the masticatory and part of the facial muscles.
At the exit from the skull, the LF is divided into two branches:
1. Sensitive ( anterior ) - innervating the mucous membranes and skin:
- cheeks, chin;
- floor of the mouth;
- lower teeth, jaw;
- lower lip, back of tongue;
- salivary glands (sublingual and submandibular);
- parts of the outer ear.
2. Motor ( posterior ) - ensuring coordinated work of muscles:
- chewable;
- maxillohyoid;
- suprahyoid;
- palatal-curtain;
- eardrum.
Classification and diagnosis of pathology
Facial nerve injuries are divided into the following types:
- neuropraxia (cured in 3-5 weeks);
- axonotmesis (moderate nerve damage, requiring up to six months of therapeutic treatment);
- neurotmesis (irreversible changes in the structure of nerve fibers. Cannot be treated with medication. Surgical intervention is required).
This neurological pathology is diagnosed using two methods:
- mechanoceptive (brush test - the patient is carried out on the lip, and the patient says the direction of movement and irritation with two points - a device resembling a mathematical compass is applied to the lower part of the face. In this case, the distance between the legs of the device is constantly increasing. As soon as the patient stops feeling each injection separately, the result is recorded and the degree of nerve damage is determined);
- nociceptive (pin prick, temperature test).
Taste buds are tested by dipping a cotton swab in salty or sweet water.
Treatment
Pain in the area of the inferior branch of the trigeminal nerve requires the use of 3 treatment methods.
Drug therapy. The doctor prescribes blockers and painkillers to reduce symptoms. The dentist will also recommend anti-inflammatory therapy. This treatment usually lasts 5-7 days.
Removing the artificial root. 1-1.5 days after implantation of the rod (if symptoms occur), dentists recommend immediately removing the implant, since such a decision increases the chances of a favorable outcome of therapy. Further treatment is carried out with medication.
Surgical intervention. Indications for a radical method are considered to be the failure of removal of the implant and treatment with medications.
Important! Removing the implant is not always the key to successful treatment of the nerve, but this action increases the chances of a quick recovery and reduces the risk of tumor formation in the area of the nerve bundle.
Treatment tactics are agreed upon with the patient, who signs consent for the operation.
Predictions and prevention
| Click to sign up for a FREE consultation |
Neuropraxia and axonotmesis are quite treatable. Statistics show that more than half of patients completely cure the disease. With neurotmesis, complete recovery does not occur.
Dentists call the main preventive measure a comprehensive study of the performance of the dental system before implantation. At the diagnostic stage, the doctor finds out the exact location of the nerve. This helps to avoid injury to the “twig”.
An experienced dentist will definitely analyze CT and X-ray data, compare the results and draw up an implantation plan based on the individual structural features of the patient’s lower jaw.
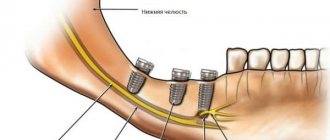
The implant is screwed in carefully; its final position should be no closer than 2 mm to the nerve process.
Damage to the mandibular nerve
Installation of dental implants in the lower and upper jaw is performed under mandibular anesthesia, which suppresses the sensitivity of nerve endings for 3-5 hours. Numbness in the lower part of the face during this period is considered normal.
Persistent loss of sensation, pain, and uncontrollable salivation suggest injury to the branch of the trigeminal nerve, which runs along the nerve canal of the mandible.
Damage is considered to be injury to one of its bundles:
- Submental: n. mentalis.
- Lingual: n. Lingualis.
- Alveolar: n. alveolaris inferior.
Has a damaging effect:
- stretching;
- compression;
- crushing;
- rupture (partial, absolute).
Injury to nerve bundles when installing an artificial dental root of the lower row leads to a decrease in the sensitivity of the innervated organs. Manifests itself in pain and numbness:
- cheeks, 2/3 tongue;
- teeth, gums;
- lower lip, part of the chin.
Loss of sensitivity of these organs makes it difficult to care for the oral cavity and facial skin, complicates eating, and sometimes disrupts facial expressions.
Causes
The NAN is damaged not only during the installation of implants, but this is the main reason. In addition to unsuccessful implantation of an artificial root, the nerve suffers in the following cases:
- extraction of incorrectly located wisdom teeth in the lower row;
- penetration of the composite material into the canal with the nerve;
- improperly performed conduction anesthesia.
Infectious diseases and inflammatory processes with suppuration also often threaten the integrity and full functionality of the inferior alveolar nerve.
Symptoms of the lesion
You can assume that the mandibular nerve is affected by the following signs:
- numbness of the face from the implantation side: lower lip, chin, tongue, lower teeth, cheeks;
- pain in the implant area;
- the appearance of profuse salivation;
- choking when eating or drinking;
- the occurrence of facial expression and articulation disorders.
A person feels discomfort when caring for facial skin (unpleasant sensations during shaving, applying makeup). Clinical manifestations depend on the type of injury and the depth of the lesion.
How is the disease diagnosed?
The diagnosis of a neurological disorder is carried out by a specialist - a neurologist. To exclude dental pathologies, an initial consultation and examination by a dentist will be required. The primary examination is carried out by palpation. The doctor determines the pain of the main points located on the tongue and in the sublingual area. Unpleasant sensations occur when pressure is applied to the skin located in the lower part of the jaw on the side in which the disorder develops. In this case, there is no change in taste sensations. Degenerative changes in the mucosa, ulcerative lesions, and deformation of the lingual papillae can be visually determined.
To clarify the diagnostic assumption, the described nerve processes are blocked. Common anesthetics are used for this: lidocaine, novocaine. Confirmation of the suspected disease occurs if the pain disappears as a result of the administration of local anesthesia. At the same time, the neurologist tries to exclude anomalies with similar symptoms: tumors, cystic processes, damage to the trigeminal nerve, etc.
Types of jaw nerve injuries
- Neuropraxia is a minor injury: benign course, favorable prognosis. In the absence of damage to the integrity of the nerve bundle, independent regeneration occurs within a month and a half.
- Axonotmesis is partial degeneration of the myelin sheath: restoration of nervous tissue is incomplete, possibly 1.5 months after damage. Medical attention is required.
- Neurotmesis - complete damage: degenerative changes in biophysical, biochemical parameters of nervous tissue. The prognosis is poor: high risk of irreversible loss of sensitivity .
Causes of inflammation
The installation of a dental implant should be carried out taking into account the parameters of the jaw, size, characteristics of the alveolar process and bone tissue of the implanted area. The relief of the canal through which the mandibular nerve bundle passes must be thoroughly studied.
Lack of preparation for implantation and lack of professionalism are the main causes of damage to the mandibular branch.
You can touch or damage the neurovascular bundle:
- needle during anesthesia;
- direct pressure with a long implant;
- tool when forming a dental bed.
Damaging factors include a long period of flap retraction and bone graft harvesting. Restoring sensitivity is a long and problematic process; the task of implantologists is to reduce potential risks to a minimum .
Injury Prevention
Prevention is high-quality preparation for surgery and professional performance of manipulations. A thorough study of the structure of the patient’s mandibular canal, the parameters of the alveolar process and the topographical position of the nerve fiber prevents neurological complications.
For this purpose the following are assigned:
- orthopantomogram;
- computed tomography - 3-dimensional scanning.
Complications will be avoided:
- correct formation of the implant bed;
- careful implantation of the dental structure;
- lateralization (change in the position of the nerve) when it is close to each other.
What methods are used in treatment
The treatment method depends on the extent of the lesion and is carried out after assessing the sensitivity deficit. With neuropraxia, recovery occurs on its own within 4-6 weeks . No medical attention is required since the nerve structure is not damaged.
With partial degeneration, symptoms subside two months after the injury. For a complete recovery, medical measures will be needed. Numbness for 9-12 months is dangerous due to irreversible degeneration of nerve cells . Microsurgical treatment can be urgent (for an open injury) or planned (for a closed injury).
Treatment tactics for closed injury
- For numbness that does not go away for three months - suturing, transplantation;
- For dysesthesia (perversion of sensitivity) for more than 3 months - revision, decompression, neurolysis, suturing and nerve transplantation;
- If hypoesthesia (decreased sensitivity) lasts for more than 3 months, partial unscrewing or removal of the structure, revision, transplantation, suturing is indicated.
Drug treatment
Indicated for chronic nerve inflammation syndrome. An important point is pain relief. Can be used:
- Antineuralgic drugs:
- Carbamazepine;
- Phenytoin;
- Baclofen.
- Antidepressants:
- Amitriptyline;
- Imipramine.
- Local products:
- ointments with capsaicin;
- acupuncture;
- electrical stimulation;
- physiotherapy.
Features of the treatment of trigeminal neuralgia
Toothache with neuralgia is a signal to immediately seek help from a neurologist. Inflammation of the trigeminal nerve is a serious problem that requires qualified assistance. Treatment of neuralgia must be comprehensive to achieve the best results in the fight against the disease.
In the process of treating neuralgia, it is important to correctly determine the cause and type of inflammation in order to be able to prescribe the appropriate treatment. When secondary neuralgia develops, before treating the main problem, it is necessary to eliminate the disease that was the cause.
To eliminate trigeminal neuralgia, specialists use therapeutic and surgical treatment methods. Most often, drug treatment is used in the form of drugs with an anticonvulsant effect, antihistamines, and vitamin therapy. However, if the use of medications is ineffective, it becomes necessary to act on the nerve through surgery.
Therapy results
The prognosis of microsurgical and therapeutic treatment is influenced by:
- age, health status of the patient;
- skill and experience of the surgeon;
- the duration of the period between injury and surgery.
In 80% of cases of neurotmesis operated on in the first 5 months after injury, partial restoration of the function of the mandibular nerve was observed. Delaying surgical intervention systematically reduces the chance of recovery. Seeing a neuromicrosurgeon a year or more after injury has only a 10% chance of success.
Still have questions? Contact us:
— Could this disease return?
— As with any dental disease, you need to be examined by a dentist every six months.
— What prevention is there for this disease?
— It is necessary to be attentive to the issue of restoring the shape of the dentition and prosthetics, treat your treatment wisely and consult with qualified specialists.
Doctor, thank you!