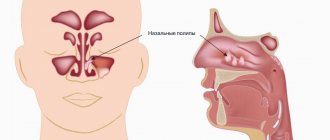
Before studying the material, we recommend that you familiarize yourself with the structure and functions of the nose.
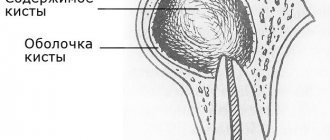
Paranasal sinus cysts are a bubble filled with fluid. The size of the cyst and its location can vary greatly. The most important thing I would like to note is that the cyst has nothing to do with oncology. This is not a neoplasm, not a tumor, it is just a bubble with a light yellow liquid. The mechanism of cyst formation is quite simple.
There are glands in the nasal mucosa. Each gland produces secretion (mucus) and has its own excretory duct, which opens on the surface of the mucous membrane. If the outflow from the gland is disrupted, a cyst forms. The gland fills with fluid and swells to a large size.
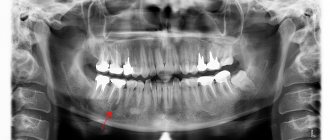
Cysts are a common disease of the paranasal sinuses. Among all types, cysts in the maxillary sinuses are the most common. Usually the cyst does not cause any complaints and is detected by chance, during an X-ray examination, computed tomography (CT) or magnetic resonance imaging (MRI), as well as when the patient takes a panoramic photograph of the upper and lower jaw - orthopantogram - when visiting a dentist. About 10% of healthy people have “silent” (not causing any symptoms) sinus cysts.
An asymptomatic maxillary sinus cyst, that is, a cyst that does not bother you, usually does not require treatment. The exception is suppurating odontogenic cysts, as well as ordinary cysts, if the dentist plans to install upper jaw implants with a preliminary sinus lift procedure. With this manipulation, the volume of the maxillary sinus can be significantly reduced, and a previously asymptomatic cyst of small size can fill the entire volume of the reduced sinus and cause pathological symptoms.
Symptoms
As mentioned earlier, a cyst in the sinus can only be seen in photographs. A regular plain x-ray of the sinuses can reveal a large cyst, but it does not always provide reliable data. A more accurate method is computed tomography. This method identifies cysts of any size and in any sinuses, and also allows you to distinguish a benign, “mucosal” cyst from an odontogenic one of dental origin, as well as from neoplasms. Magnetic resonance imaging (MRI) is not very good at assessing the sinuses and often exaggerates the extent of the pathology. Therefore, the ideal image for diagnosing the condition of the paranasal sinuses today is a computed tomogram (CT).
The most common symptoms of a cyst in the sinus are: pain and a feeling of pressure, fullness, a sensation of a foreign body, usually on one side, in the projection of the sinus, repeated inflammation of the sinus (sinusitis, frontal sinusitis, sphenoiditis), less often nasal congestion. These symptoms intensify more often during a cold, during an airplane flight, or when tilting the head down. The most pronounced symptoms are with cysts in the sphenoid sinuses, which are located at the base of the skull. In addition to complaints of intense, often occipital pain, patients note double vision or blurred vision, and sometimes they experience epileptic conditions. The pain symptom is associated with the pressure of the cyst on the walls of the sinus, with its sensitive nerve endings, and the inflammatory phenomena are associated with a block of ventilation anastomosis and a violation of the outflow of secretions.
Sometimes patients complain of a feeling of pressure under the eye. Sometimes the cyst grows and completely fills the entire maxillary sinus and even extends into the nasal cavity, blocking nasal breathing - with the formation of a choanal polyp. In such a situation, as a rule, the maxillary sinus has an additional anastomosis with the nasal cavity, the correct drainage of mucus is disrupted - its constant recirculation occurs, as a result of which first a cyst is formed, and then a polyp.
Make an appointment online
Without queues and long waits, at a time convenient for you to see any doctor
Sign up
What is a cyst in the maxillary sinus called?
A maxillary sinus cyst is a benign formation that has a hollow structure containing fluid inside. Cysts of the maxillary sinuses are quite common, but are almost always found at random. Their location and origin may differ, which will determine the characteristics of the clinic and even treatment.
Odontogenic cyst
Among the many benign tumors of the jaw tissue, the cyst is found most often and represents a pathology quite dangerous for the bone structure. Odontogenic formations in the vast majority of cases remain undiagnosed for a long time, and therefore reach enormous sizes. The growth of the cyst provokes atrophic processes in the bone tissue, which thins, becomes fragile, and then disappears completely.
Such formations are characterized by a long latent course until the cavity grows to gigantic proportions. Then a characteristic crunch begins to be noted in the jaw, especially during chewing loads. Ignoring the problem leads to spontaneous fractures of the jaw, compression of the maxillary sinus with disruption of its functions, exacerbation of the inflammatory process with damage to the structures of the maxillary sinus and the formation of sinusitis.
Tooth cyst growing into the maxillary sinus
Damage to the dental canal involving the root and surrounding tissues is a consequence of an infectious process of bacterial origin. In the absence of adequate and timely treatment, a gradual delimitation of the inflammatory reaction from healthy tissues by a wave of cellular structures occurs.
This creates a cavity called a dental cyst. It gradually increases and destroys the bone tissue of the jaw. When localized in the anterior part of the upper jaw, gradual penetration into the maxillary sinus occurs.
Retention
The most common form of neoplasm in the maxillary sinus, which is also called a true cyst. It is located in the lower wall of the sinus and has an epithelial lining - a distinctive feature of true cystic cavities. The formation is clearly determined by X-ray examination randomly, as it does not manifest itself clinically.
When the cyst reaches a significant size, problems begin with the functioning of the maxillary sinus. The structure and physiology of the microvasculature is disrupted, resulting in the formation of edema. This symptom is manifested by nasal congestion, often without pronounced discharge from it. Due to the lack of specificity of the clinical picture, even the presence of subjective signs of the disease is not a reason to consult a doctor.
Treatment
Treatment of the cyst comes down to two alternatives: surgical removal (if indicated) or passive observation of the patient. The cyst is removed if it causes concern.
There are two main approaches for removing a cyst - through the anterior wall of the sinus (an incision under the lip just above the gum) and through the nasal cavity.
The essence of the first operation , the so-called radical Caldwell-Luc operation, is as follows: an incision is made under the lip, after which the anterior wall of the sinus is opened and the cyst is removed through the resulting hole. The operation is quite traumatic, which is of significant importance in the postoperative period. This type of operation was previously classical and was often used. With the introduction of endoscopic methods into practice, radical surgery was replaced by microsinusrotomy (MGT), also performed through the anterior wall of the sinus, but without a preliminary incision, using a special Kozlov trocar instrument. The operation takes no more than 5 minutes, is low-traumatic, and is very effective for cysts of the maxillary sinuses, when the surgeon does not intend to expand the natural sinus anastomosis.
The second method, although considered more modern and progressive, is, unfortunately, also traumatic. It is also endoscopic, but is performed through the nasal cavity with preliminary expansion of the natural anastomosis of the maxillary sinus, which is not justified in all cases. It is most often used for choanal polyps and common polypous rhinosinusitis.
It must be remembered that sinusitis in most cases is not a problem of the maxillary sinus itself. 90% - look for a problem in the nasal cavity, 10% - look for a problem with the teeth. Currently, the proportion of odontogenic (dental) sinusitis is progressively growing. And therefore, most often, for complete treatment, it is not enough to remove only the cyst from the sinus; it is necessary to immediately eliminate the cause that caused its appearance. Most often, correction of the curvature of the nasal septum, surgery on the nasal turbinates and in the area of the ethmoid labyrinth are required, the purpose of which is to restore normal ventilation of the nose and its paranasal sinuses. This tactic allows you to prevent relapses of cysts and chronicity of the inflammatory process.
Pathogenesis
The pathogenesis of paranasal sinus cysts varies depending on the type of cyst. Thus, true cysts are formed when the lumen of the ducts of the glands of the sinus mucosa is obliterated due to squamous metaplasia of their epithelium and disruption of the process of outflow of their secretions. They develop against the background of inflammatory reactions caused by blockage of the lumen of the excretory duct with necrotic masses and stretching of the tissues of the gland and the proximal part of the duct. The leading mechanism of cystic transformation of the glands is a change in the composition of the secretory epithelium and hyperplasia of the glands. It is based on a sharp mucoidization of the secretory epithelium. At the same time, serous elements undergo pronounced changes, which, against the background of high mucoidization, are completely reduced. The corresponding transformation of the structure of the glands, together with goblet cell hyperplasia, leads to disruption of the transport function of the mucosa, excessive accumulation of secretions in the terminal sections of the glands, followed by cystic expansion, gradual enlargement and fusion into one common cavity. Also, the formation of cysts may be preceded by compression of the gland and duct by connective tissue.
False cystic formations develop primarily as a result of progressive disorganization of connective tissue (edema, degenerative changes in the mucosa and morphologically confirmed separation of connective tissue). At the same time, the leading role in the development of false cysts belongs to immunopathological mechanisms, as evidenced by the cellular composition of inflammatory infiltrates (eosinophils/mature plasma cells) and the predominant damage to blood vessels.
Odontogenic radicular cysts of the maxillary sinuses develop as a result of epithelial granulomas/necrotic changes in the apical part of a tooth affected by caries in combination with atrophic processes in the bone of the upper jaw. The development of follicular cysts is based on inflammatory lesions of the impacted tooth germ of primary teeth. Congenital cysts develop against the background of various developmental anomalies of glandular tissue/ducts of the mucous glands.
What operations are performed for maxillary sinus cysts?
Currently, cysts of the paranasal sinuses are removed along with their walls. The previously practiced puncture with suction of the contents of the cystic cavity does not give the desired effect. After all, the glandular cells remaining in the walls of the cyst will continue to function, which will lead to relapse.
Removal of a maxillary sinus cyst can be done in several ways:
- surgical intervention according to Caldwell-Luke, with opening (trepanation) of the wall of the maxillary sinus through an intraoral incision under the upper lip; until recently, such an operation was considered the “gold standard” for the treatment of maxillary cysts of any origin;
- surgery with Denker access - the sinus is opened through a soft tissue incision running along the nose, used for large posterior cysts;
- endoscopic cyst removal.
Significant disadvantages of classical surgical techniques are their high invasiveness, long period of tissue healing, and the need for general anesthesia (anesthesia) and hospitalization. Therefore, endoscopic removal of maxillary sinus cysts is currently preferred. After all, this technique refers to gentle microinvasive interventions and is performed on an outpatient basis, under local anesthesia.
Where to undergo surgery to remove a sinus cyst?
"European Clinic of Dr. Savinkov" is one of the flagships in Russian endoscopic nasal surgery for functional (FESS-surgery) indications. Rhinological surgeons and medical staff of the clinic constantly improve and maintain their professional level, offering their patients treatment at the level of the best world standards.
Modern endoscopic technologies for nasal surgery used in our clinic make it possible to remove a cyst from the maxillary sinus non-traumatically, without incisions on the face, physiologically, and painlessly. The method has virtually no contraindications. The duration of the operation is 20-40 minutes. The hospital stay is 2-3 hours.
We operate on patients from Chelyabinsk, Moscow, Yekaterinburg, Magnitogorsk, Kurgan, Tyumen, Surgut and other cities.
The cost of surgical treatment of maxillary sinus cysts is clarified during consultation, after an endoscopic examination of the nasal cavity. You can find out the estimated cost of treatment from an ENT surgeon by calling the numbers listed below or via instant messengers.
Telephones in Chelyabinsk:
sign up for a consultation
chief surgeon,
Phone in Moscow:
List of sources
- Zakharova, G.P. Clinic, pathogenesis and surgical rehabilitation of patients with cyst-like formations of the maxillary sinuses / G.P. Zakharova // Sat. scientific tr. XV Congress of Otorhinolaryngologists of Russia. - St. Petersburg, 1995.-T. 1.-S. 96-102.
- Daynyak, L.B. Nose and paranasal sinuses / L.B. Daynyak // Guide to otorhinolaryngology. M.: Medicine, 1994. - P. 222.
- Guryev I.S., Dolzhikov A.A. Features of patho- and morphogenesis of cysts of the paranasal sinuses. Russian rhinology. 2002; 2:53-54.
- Allahverdiev S.A., Lopatin A.S. Choosing the optimal surgical approach for maxillary sinus cysts. Russian rhinology. 2010;(1):34-35.
- Kulakov A. A. Surgical dentistry and maxillofacial surgery. National leadership / ed. A. A. Kulakova, T. G. Robustova, A.I. Nerobeeva. - M.: GEOTAR-Media, 2010. - 928 p.
Prevention
If treatment and surgery to remove a maxillary sinus cyst were carried out on time, complete recovery occurs in 90% of patients. Some risk of developing a recurrent defect remains, but much depends on the appearance of a new source of infection. If treatment is delayed for a long time, complications are possible, the spread of pus, breakthrough of formation, development of phlegmon. All of these are dangerous conditions.
Prevention consists of timely treatment of teeth, nasal diseases (septum correction, treatment of inflammatory processes) and allergic diseases.
A CYST CAN ONLY BE CURED WITH SURGICAL INTERVENTION
CARRYING OUT THE OPERATION
Cyst removal is possible in two ways: classical and endoscopic.
The first method is more traumatic, since the sinus wall is surgically opened over a wide area.
The endoscopic technique used at Medical Plaza MC is a new, progressive, minimally invasive method aimed at removing cysts from the maxillary sinus, which leaves minimal physiological consequences for the body.
The operation can be performed under general or local anesthesia. The intervention takes place through a natural opening in the nasal cavity. Through it, the cyst is removed and the patient can be discharged from the hospital the very next day. After removal of the cyst, the patient is under the supervision of an otolaryngologist to prevent recurrence