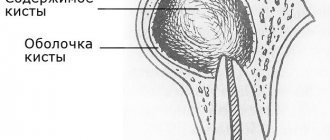
A radicular cyst is a cavity formation at the apex of a tooth root. The inside is lined with epithelial tissue and filled with cystic fluid. The most common cause of a radicular cyst is chronic periapical inflammation. The disease is often asymptomatic and is detected only during a dental examination or x-ray of nearby teeth.
Causes of radicular cysts
The development of a radicular cyst in most cases is caused by an infectious-inflammatory process. The body forms a cystic formation to isolate the source of infection. The inflammatory process begins due to:
- chronic untreated caries;
- pulpitis;
- granulomatous periodontitis (over time, granulomas transform into cysts);
- tooth or jaw injuries;
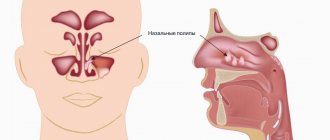
- previous infectious disease (angina, otitis, sinusitis);
- reduced immunity;
- malocclusion;
- complications during the eruption of wisdom teeth.
Prevention
Radicular cyst is a serious disease, the treatment of which is traumatic, and the recovery period lasts for a long time. The peculiarities of the clinical course of the disease do not allow one to independently suspect it at an early stage, since the formation does not make itself felt. That is why we recommend visiting the dentist twice a year. The specialist will detect caries in time and carry out dental treatment, preventing the occurrence of complications that could cause the formation of a cyst. If there is the slightest suspicion of a radicular cyst, the doctor will conduct an X-ray examination to confirm or exclude the diagnosis.
Oral hygiene is an important measure for the prevention of many dental diseases, including radicular cysts. Timely removal of plaque creates unfavorable conditions for the development of bacteria in the oral cavity. Those who regularly brush their teeth and remove food particles between their teeth after eating have the least chance of becoming a victim of this serious disease.
Strengthen your immune system and promptly sanitize chronic foci of infection in the body, visit the dentist regularly. This is the key to the health of your teeth.
Symptoms
The disease has no pronounced symptoms. Minor signs that are sometimes observed are attributed by patients to other pathologies and ignored. When examining the oral cavity, a dentist may suspect a cyst when he discovers a darkened tooth or advanced caries. If you probe the root canals, a yellowish liquid discharge and absence of pain during manipulation will indicate a cyst.
The formations can reach 5 cm in diameter. With significant dimensions of the radicular cyst, displacement of the teeth occurs; upon palpation in the affected area, pliability and a “parchment crunch” are felt.
The cyst develops asymptomatically until it suppurates. It is accompanied by pain localized around one tooth, weakness, and fever.
Sometimes the infection spreads to the inner ear and sinuses, causing an acute inflammatory process. A large cyst can deform the walls of the maxillary sinus, cause atrophy of the spongy bone and sinusitis.
Cost of treating a cyst under a tooth
The price of dental services for the treatment of cysts in our clinic is about 8,500 rubles. and depends on the following factors:
- type;
- complexity of the disease;
- method of treatment (surgical or therapeutic);
- use of complex equipment;
- expenses for surgical or dental supplies;
| Service | Price |
| Consultation | For free |
| Orthopantomogram OPTG of the jaw | from 1,100 ₽ |
| Cystectomy | 5 300 ₽ |
| Hemisection | 3 300 ₽ |
Look at the detailed price list for dental treatment at NovaDent dentistry in Moscow and the pain-free region.
If you have been diagnosed with a dental cyst, it should be treated by a qualified dentist. Many patients do not fully understand the danger of this disease. Photos of the cyst can be found on the Internet. From them it can be understood that this can cause the destruction of large areas of bone tissue. And this, in turn, poses a risk of jaw fracture and tooth loss.
Expert of the article you are reading: Svetlana Viktorovna Derevyakina Chief physician, doctor of the highest qualification category, therapist, periodontist, leading specialist of the NovaDent network
27 years
Clinical experience
Petrovsko-Razumovskaya
Verkhniye Likhobory
st. Dubninskaya, 27, building 1
+7
Free consultation with this specialist
Diagnostics
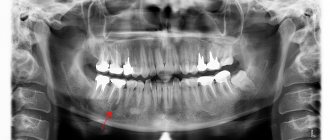
Often a cyst is found when neighboring teeth begin to be treated. A radicular cystic formation is clearly visible on an x-ray - it is a round-shaped shadow with a clear border, adjacent to the apex or wall of the root.
To clarify the diagnosis, electroodontometry is done. To clarify the nature of the neoplasm, a puncture with a thick needle is prescribed. To check the extent and distribution, you will additionally need radiography of the paranasal sinuses, sometimes contrast radiography and computed tomography of the upper jaw bone.
Treatment
Radicular cysts are treated through surgery—cystotomy or cystectomy.
Cystotomy is used in the case of a large cyst that affects the roots of several adjacent teeth and destroys the walls of the maxillary sinus. The operation involves cleaning out the cyst cavity through a small hole made from the mouth, nose or paranasal sinus. Upon completion, the surgeon disinfects the cavity and inserts a swab with iodoform there. A week later, the tampon is replaced with a new one, and this continues until the doctor is convinced that the inflammatory process has stopped.
Cystectomy is the removal of a cyst by separating the fibrous membrane of the formation from the surrounding tissue. The operation ends with tamponade of the cavity or bringing together the edges of the mucous membrane that have been damaged. Cystectomy is done for small cysts.
Postoperative recovery will be successful if the patient takes oral hygiene instructions seriously: use antiseptic rinses and brush teeth carefully. In case of increased body temperature, as well as intense and prolonged pain, you should immediately consult a doctor.
FEATURES OF TREATMENT OF RADICULAR CYSTS OF THE JAW BONESDepartment of Hospital Surgical Dentistry and Maxillofacial Surgery of Moscow State Medical University.
Head of the department, professor Drobyshev A.Yu.
Asnina S.A. Kokota N.B. Drobyshev A.Yu. Ivanova E.S.
Summary. The goal of surgery for jaw bone cysts is to preserve teeth and restore their function. The article describes methods of surgical intervention using biocomposite materials to solve the problems.
Key words: radicular cyst, directed regeneration, retrograde filling, biocomposite material.
Introduction. Radicular cysts of the jaw bones account for 7 to 12% of all diseases of the maxillofacial region. The main goal of surgical treatment of perihilar cysts of the jaws is to preserve the teeth located in the cyst area and restore their function.
Among the operations performed by dental surgeons on an outpatient basis, operations for radicular cysts of the jaws take second place after tooth extraction (M.M. Solovyov et al., 2004).
The growth of the cyst is caused by a number of factors: the pressure of the accumulated exudate, the growth of granulation tissue and differentiation of its elements, and finally, the growth of the epithelium lining the cyst cavity (G.D. Ovrutsky et al., 1999). The direction of cyst growth depends on the density of the bone tissue and the location of the roots of the causative tooth in relation to the vestibular cortical plate of the jaw. As a rule, the bone tissue is thinned in the area of the buccal root of teeth 1.4, 2.4, and the buccal roots of teeth 1.6 and 2.6. In the area of these teeth, cysts tend to destroy the cortical plate and extend beyond the bone tissue, under the periosteum. Such radicular cysts are called “subperiosteal” cysts.
Clinically, the subperiosteal cyst has the appearance of a spherical neoplasm at the level of the causative root.
Rice. 1. Subperiosteal cyst of the anterior buccal root of tooth 1.6
An X-ray examination often reveals an expansion of the periodontal fissure, or a slight loss of bone tissue in the area of the apex of the root of the causative tooth.
Rice. 2. Orthopantomogram of patient L. There are no visible changes in the area of the apex of the anterior buccal root of tooth 1.6.
After infiltration anesthesia, at a distance of 3-5 mm from the neoplasm, an arcuate incision is made and the mucoperiosteal flap is peeled off. There is no bone tissue above the shell.
A
b
V
G
d
e
Rice. 3. Stages of surgical intervention: a. The mucoperiosteal flap is detached; b. The probe enters the canal of the anterior buccal root by 3 mm; V. Obturation of the anterior buccal root of tooth 1.6 with “Adhesor fine” cement; g. Membrane "Osteoplast"; d. The wound was sutured with catgut; e. Septopac dressing.
The arrow indicates the membrane of the cyst. The size of the bone defect corresponds to the size of the cyst. After removing the cyst shell, the root is resected at an angle of 30 degrees for better access to the canal.
Probing revealed a lack of filling material in the canal. The entrance to the canal is expanded, the formed cavity is filled with cement.
For targeted regeneration of bone tissue, the absorbable membrane “Osteoplast” was used. After mobilization, the flap is placed in place and sutured with catgut. The operation ends with the application of a bandage.
After detachment of the mucoperiosteal flap, the absence of the vestibular cortical plate along the entire length of the root is often discovered. As a rule, such teeth must be removed. To preserve the tooth, it is necessary to fill the postoperative bone cavity with a biocomposite material and use a resorbable membrane for targeted regeneration of bone tissue.
In patient A. tooth 4.4 is a support in the orthopedic structure, the tooth canal is sealed to the apex.
Rice. 4. Fragment of an orthopantomogram of patient A. Radicular cyst of the lower jaw in the area of tooth 4.4.
To save tooth 4.4, a cystectomy operation is planned with filling the bone defect with bio-composite material.
A
b
V
G
Rice. 5. Stages of the operation: a. The cyst membrane was removed. The vestibular cortical plate is completely absent; b. The bone cavity is filled with biocomposite material.; V. Resorbable membrane "Osteoplast"; d. The operation is completed. The seams are catgut.
The cyst shell was completely removed, the bone at the root apex was treated with a spherical bur. Resection of the root of tooth 4.4 is not indicated. To prevent mucosal ingrowth into the bone cavity, it is necessary to use a resorbable membrane. As can be seen from the figures, the patient underwent cystectomy without resection of the root of tooth 4.4. The postoperative defect is filled with the biocomposite material “Osteoplast-K”, and the resorbable membrane “Osteoplast” is used.
Conclusion. The main goal of surgical treatment of perihilar cysts of the jaws is to preserve the teeth located in the cyst area and restore their function. After removal of perihilar cysts, bone cavities remain, which reduce the strength of the jaw bones and can cause functional and aesthetic problems. In addition, with standard surgery, the blood clot filling the bone defect is reduced, which leads to infection of the bone cavity and subsequent complications.
The problem of preventing postoperative inflammatory complications after cystectomy has received insufficient attention in the literature. The use of biocomposite materials to fill a bone defect after surgery is the main method in the prevention of postoperative complications. Bone tissue regeneration is a long process; in the absence of a vestibular cortical plate, the mucoperiosteal flap tends to fill the available space, which prevents bone restoration. Filling a bone defect with a biocomposite material and using a resorbable membrane promotes targeted regeneration of bone tissue.
Conclusions:
1. The main goal of cystectomy is not only to preserve the tooth that was previously removed, but also to restore its function.
2. Resection of the root apex to the vestibular side at an angle of 30 degrees is indicated if retrograde root filling is necessary.
3. Filling a postoperative bone defect with a biocomposite material is a method of preventing postoperative complications.
4. In the absence of a cortical plate, a resorbable membrane must be used for directed regeneration of bone tissue.
Literature:
1. Abdalov Kh.B. //Increasing the effectiveness of treatment of destructive forms of chronic periodontitis//. Author's abstract. dis. Ph.D., M., 1990. p. 15.
•2. Asnina S.A., Agapov V.S., Volozhin A.I., Belozerov M.N., //Surgical treatment of chronic foci of inflammation in periodontal tissues. // Materials of the V International Conference of Maxillofacial Surgeons and Dentists. St. Petersburg, 2000, p.2
3. Asnina S.A., Ivanova R.S., Emelyanova E.A. //Surgical treatment of foci of odontogenic infection in periodontal tissues//. Proceedings of the conference dedicated to the 100th anniversary of the birth of Professor E.E. Platonov. M. 2001, 168-170.
4. Borovsky E.V., Zhokhova N.S. //Endodontic treatment//. M., 1997..p.63.
5. G.D. Ovrutskiyts, Yu.N. Livshits, L.M. Lukins. “Non-operative treatment of perihilar cysts of the jaws,” M. 1999.
•6. MM. Soloviev, G.M. Semenov, D.V. Galetsky “Surgical treatment of odontogenic cysts”, S-P-, 2004.