An ovarian cyst is a fluid-filled sac that forms on the tissue of one or both ovaries.
All such formations are divided into functional and organic. The first are the result of a short-term malfunction of the organ, when the follicle does not rupture at the right time and does not release the egg. Cysts of this type either go away on their own within a month or are easily treated with hormonal medications. Organic cysts are more difficult to treat and may require surgery. In addition, cystic tumors can be either benign (mucinous and serous cystadenomas, dermoid cyst, cystedenofibroma, and sclerosing stromal tumor) or malignant (serous and mucinous cystadenocarcinomas, Brenner cystic tumor, endometrioid carcinoma, cystic metastasis, and immature theroma).
Get an MRI of the pelvis in St. Petersburg
It is believed that ovarian cysts can result from:
- Early onset of menstruation;
- Hormonal disorders in the thyroid gland;
- Abortion and other methods of termination of pregnancy;
- Various diseases of the reproductive system;
Types of ovarian cysts in women
There are main types of ovarian cystic formations:
Physiological cysts are normal
- Follicle
- Corpus luteum
Functional cysts
- Follicular cyst
- Corpus luteum cyst
- Thecal lutein cysts
- Complicated functional cysts: hemorrhagic cyst, rupture, torsion
Benign cystic tumors (cystoma)
- Dermoid cyst (mature teratoma)
- Serous cystadenoma
- Cystadenoma mucinous
- Cystedenofibroma
- Sclerosing stromal tumor
Malignant cystic tumors (cystomas)
- Serous cystadenocarcinoma
- Cystadenocarcinoma mucinous
- Endometrioid cancer
- Brenner's cystic tumor
- Immature teratoma
- Cystic metastasis
Other cysts
- Endometrioma (chocolate cyst)
- Polycystic ovaries (Stein-Leventhal syndrome)
- Postmenopausal cyst
- Ovarian hyperstimulation syndrome
Normal anatomy and physiology of the ovaries during reproductive age
Before considering pathological changes, we will highlight the normal anatomy of the ovary. A woman's ovary at the time of birth contains over two million primary oocytes, about ten of which mature during each menstrual cycle. Despite the fact that about a dozen Graafian follicles reach maturity, only one of them becomes dominant and reaches a size of 18–20 mm by the middle of the cycle, after which it ruptures, releasing the oocyte. The remaining follicles decrease in size and are replaced by fibrous tissue. After the oocyte is released, the dominant follicle collapses, and granulation tissue begins to grow in its internal lining in combination with edema, resulting in the formation of the corpus luteum of menstruation. After 14 days, the corpus luteum undergoes degenerative changes, then a small scar remains in its place - the white body.
Graafian follicles: small cystic formations found in the structure of the ovary normally in all women of reproductive age (premenopausal period). The size of the follicles varies depending on the day of the menstrual cycle: the largest (dominant) usually does not exceed 20 mm in diameter at the time of ovulation (14th day from the start of menstruation), the rest do not exceed 10 mm.
Ultrasound of the ovary is normal. Sonograms show ovaries containing several anechoic simple cysts (Graafian follicles). Follicles should not be confused with pathological cysts.
What do the ovaries look like on an MRI? On T2-weighted MR images, Graafian follicles appear as hyperintense (i.e., bright signal) cysts with thin walls surrounded by ovarian stroma, which gives a less intense signal.
Normally, in some women (depending on the phase of the menstrual cycle), the ovaries can intensively accumulate radiopharmaceuticals (RP) during PET. To distinguish these changes from a tumor process in the ovaries, it is important to correlate them with the patient’s anamnestic data, as well as with the phase of the menstrual cycle (the ovaries intensively accumulate radiopharmaceuticals in the middle). Based on this, it is better for women before menopause to be prescribed PET scans in the first week of the cycle. After menopause, the ovaries practically do not take up radiopharmaceuticals, and any increase in its accumulation is suspicious for a tumor process.
PET-CT of the ovaries: increased accumulation of a radiopharmaceutical (RP) in the ovaries of a woman in the premenstrual period (normal variant).
Is it possible to get rid of a cyst without visiting a doctor?
Dental treatment has long ceased to cause severe pain, which has become possible thanks to the development of medical technology, but many people still do not like the hassle of going to the dentist, delaying the visit until the last minute.
A person who notices a cyst often tries to get rid of it with the help of strong antibiotics, hoping that the drugs will eliminate pathogens and stop the inflammatory process. However, none of the most modern medications will change the situation for the better if you do not get rid of the infected tissue, treat the root canals with an antiseptic and do not seal them thoroughly. Yes, antibiotics are also needed, but they play the role of an auxiliary, not a primary remedy.
All other traditional methods of treatment (applying lotions, rinsing with various solutions, using homeopathy) bring temporary relief and do not solve the problem. The pain may subside, and the cyst may even decrease slightly for a while, but the inflammatory process will continue to progress.
An abscess is quite insidious because it can develop over a long period of time without any symptoms at all. Dentistry knows many examples when a cyst grew to enormous sizes, turning into a pus-filled sac 6 cm in diameter. In such advanced cases, saving the tooth becomes extremely problematic.
Ovaries after menopause
Entering the postmenopausal period is defined as the absence of menstruation for one year or more. In Western countries, the average age of menopause is 51–53 years. In postmenopause, the ovaries gradually decrease in size and Graafian follicles stop forming in them; however, follicular cysts may persist for several years after menopause.
On a T2-weighted MR image (left) of a postmenopausal woman, the ovaries appear as dark “clumps” located near the proximal end of the round ligament. On the right, the tomogram also visualizes a hypointense left ovary, devoid of follicles. Although it is slightly larger than expected, overall the ovary appears completely normal. And, only if it is possible to detect an increase in the size of the ovaries compared to the initial study, the differential diagnostic series should first of all include a benign neoplasm, for example, fibroma or fibrothecoma.
Rehabilitation
The oncology clinic of the Yusupov Hospital has all the conditions for successful rehabilitation, which lasts from 10 days to a month. All actions during this period are aimed at restoring the reproductive functions of the body, preventing relapse of the disease, as well as normalizing the psycho-emotional state of the patient.
The rehabilitation program of the Yusupov Hospital includes several stages:
- Taking hormonal drugs;
- Phonophoresis;
- Diet correction;
- Laser or magnetic laser therapy;
- Physiotherapy.
During this time, it is necessary to abstain from sexual intercourse, heavy physical activity, and sports. After the end of the rehabilitation period, the woman can return to her usual lifestyle.
Functional ovarian cysts
Much more common are benign functional ovarian cysts, which are Graafian follicles or corpus luteum, which have reached significant sizes, but otherwise remain benign. In the early postmenopausal period (1–5 years after the last menstrual period), ovulatory cycles may occur, and ovarian cysts may also be detected. And even in late menopause (more than five years after the end of the menstrual period), when ovulation no longer occurs, small simple cysts can be found in 20% of women.
What is a functional ovarian cyst? If ovulation has not occurred and the wall of the follicle has not ruptured, it does not undergo reverse development and turns into a follicular cyst. Another variant of a functional cyst is an enlargement of the corpus luteum with the formation of a corpus luteum cyst. Both formations are benign and do not require drastic measures. An expert second opinion helps distinguish them from malignant variants.
Tooth cyst: treatment
Treatment can be divided into therapeutic (use of drugs) and surgical (gum incision and root resection).
Conservative treatment is justified if:
- no unsealing required;
- if the canal is unsatisfactorily sealed along its entire length;
- if the diameter of the cyst is large (over 1 cm), which is accompanied by pain and swelling noticeable even to a non-specialist.
Surgery is recommended when:
- there is a pin in the channel;
- there is a crown on the causative tooth;
- the root canals are unsealed at the upper part of the root for 1/3 of their length;
- The gums swell, which is accompanied by pain.
Follicular cysts
In some cases, ovulation does not occur and the dominant Graafian follicle does not undergo reverse development. When it reaches a size greater than 3 cm, it is called a follicular cyst. These cysts are usually 3–8 cm in size, but can be much larger. On ultrasound, follicular cysts appear as simple, unilocular, anechoic cystic formations with a thin and smooth wall. In this case, neither lymph nodes accumulating contrast, nor any soft tissue component of the cyst, nor septa that enhance with contrast, nor fluid in the abdominal cavity (except for a small physiological amount) should be detected. During follow-up studies, follicular cysts may resolve on their own.
Removal or treatment of a dental cyst?
The question is of great importance for people who are afraid of dental operations.
Before deciding on a treatment method, you need to consider a number of nuances:
- if you treat the cyst with medication, it will take at least 3 months; in case of surgical intervention, you will have to visit the doctor only 3-4 times;
- Nowadays, in most surgical operations, a laser has replaced the scalpel, but in some cases it is still impossible to do without traditional incisions;
- if there are deep cracks on the tooth, you cannot do without surgical intervention - no modern medications will help in this case;
- Regardless of the chosen treatment method, the probability of cyst recurrence is about 10%.
In any case, the final decision regarding the method of treatment remains with the doctor, who, based on the analysis of the x-ray and other measures, can make the right choice about the development of the disease.
Corpus luteum cyst
The corpus luteum can become obliterated and fill with fluid, including blood, resulting in the formation of a corpus luteum cyst.
Ultrasound: corpus luteum cyst. Small complex ovarian cysts are visible with blood flow in the wall, which is detected by Doppler ultrasound. Typical circular blood flow during Doppler examination is called the “ring of fire.” Note the good permeability of the cyst to ultrasound and the absence of internal blood flow, which correlates with the changes characteristic of a partially involuted cyst of the corpus luteum
It should be noted that women taking hormonal oral contraceptives that suppress ovulation usually do not develop a corpus luteum. Conversely, the use of drugs that induce ovulation increases the chance of developing corpus luteum cysts.
Pelvic ultrasound: corpus luteum cyst. On the left, the sonogram shows changes (“ring of fire”), typical of a corpus luteum cyst. On the right, in the photo of the ovarian specimen, a hemorrhagic cyst with collapsed walls is clearly visible.
Corpus luteum cyst on MRI. An axial T2-weighted tomogram reveals a cyst of the involuted corpus luteum (arrow), which is a normal finding. The right ovary is unchanged.
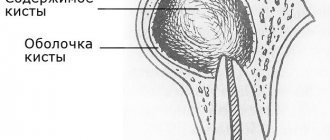
Reasons for appearance
The exact cause of a cyst on the cervix, the so-called. "Ovuli Naboti", still not installed. The Nabothian glands, located in the body of the cervix, secrete a special secretion that protects a woman’s internal genitalia from infections. If an inflammation process begins in the cervical canal or vagina, it can seize the excretory ducts of the glands, leading over time to their blockage and, as a consequence, to disruption of the excretion of the mucous secretion produced. Constantly filled in the absence of outflow, the glands begin to increase in volume and protrude above the mucous membrane of the cervix in the form of tubercles and balls. This is the mechanism of occurrence of Nabothian cyst.
Provoking factors:
- colpitis, cervicitis,
- salpingoophoritis, endocervicitis,
- trauma to the cervical canal during childbirth, abortion,
- wearing an IUD,
- diagnostic curettage,
- erosion or ectopia,
- hormonal imbalance.
Why are Ovuli Naboti dangerous, why is it better to get rid of them, even if they don’t bother you? During the next examination, the doctor made this diagnosis and the question arose before you - what should be done? It is best to remove cervical cysts, especially multiple ones, by opening them up and performing a “cauterization” operation, preferably using the radio wave method, since very often a purulent infiltrate can form in large and multiple retention formations.
Photo of cervical cyst
Nabothian gland cysts on the cervix, photographs of which can be seen below, were found in young girls and women who have already given birth. The findings were made by a gynecologist during an initial gynecological examination of patients who came to the clinic for completely different problems. This confirms the statistical data on the predominantly random discovery of ovuli naboti, a common pathology of the internal genital organs.
| The photo shows a healthy neck | Small cysts on the cervix, in the photo they look like a ball | Large Nabothian cysts |
| Many endocervical cysts | Large cysts of the cervix, in the form of tubercles | Large Nabothian cysts |
Hemorrhagic ovarian cysts
A complex hemorrhagic ovarian cyst is formed by bleeding from a Graafian follicle or follicular cyst. On ultrasound, hemorrhagic cysts appear as single-chamber thin-walled cystic structures with the presence of fibrin strands or hypoechoic inclusions, with good permeability to ultrasound. On MRI, hemorrhagic cysts are characterized by high signal intensity on T1 FS scans, while on T2 WI they give a hypointense signal. With Doppler ultrasound, there is no internal blood flow; the component accumulating contrast inside the cyst is not detected on CT or MRI. The wall of a hemorrhagic cyst has variable thickness, often with the presence of vessels located in a circular pattern. Despite the fact that hemorrhagic cysts usually manifest with acute pain symptoms, they can be an incidental finding in a patient who does not present any complaints.
Sonograms reveal a hemorrhagic cyst with a blood clot simulating a neoplasm. However, Doppler ultrasound did not reveal internal blood flow in the cyst, and its permeability to ultrasound was not reduced.
MRI picture of a hemorrhagic ovarian cyst: in the T1 VI mode without fat suppression, a complex cyst is determined, characterized by a hyperintense signal, which can be caused by both the fatty component and the blood. On T1 fat-suppressed imaging, the signal remains hyperintense, allowing confirmation of the presence of blood. After administration of gadolinium-based contrast, no contrast enhancement is observed, which allows us to confirm the hemorrhagic nature of the ovarian cyst. In addition, it is necessary to include endometrioma in the differential diagnostic range.
Ultrasound reveals a soft tissue (solid) component in both ovaries. However, ultrasound permeability on both sides is intact, suggesting the presence of hemorrhagic cysts. Dopplerography (not shown) shows no blood flow in the formations.
How to distinguish a hemorrhagic cyst on MRI? In T1 mode, a component with high signal characteristics (fat, blood or protein-rich fluid) is detected in both formations. With fat suppression, the signal intensity does not decrease, which generally makes it possible to exclude a teratoma containing adipose tissue and confirm the presence of hemorrhagic fluid.
Description of therapeutic method of treatment
This method takes a lot of time, requiring a lot of patience from the patient (you will have to visit the dentist more than once), a lot of free time and significant financial expenses.
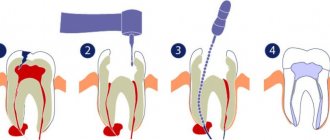
The process consists of a number of sequential stages:
- First, the doctor works with the canals. The dentist looks to see if they have been filled: if not, the pulp is removed, and the canals are processed using the instrumental method; if they were, then they need to be unsealed before proceeding with subsequent actions.
- The cyst contains pus, which is why after unsealing and getting rid of the pulp, repeated thorough rinsing of the canal with an antiseptic solution will be required.
- A potent medicine is removed from the apex of the root.
- The canal is temporarily filled with a paste that has an antiseptic effect.
- Since the medicine needs to be changed once every certain period of time, the patient will have to come to the dentist every time for this over the next couple of months. After the next change of medication, the canal is again filled with medicinal paste.
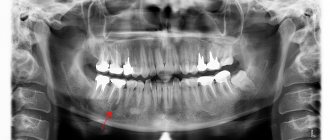
- From time to time, an x-ray is taken to monitor the progress of treatment and evaluate its progress. If the cyst in the picture becomes smaller over time, then this indicates positive dynamics.
- When the cyst shrinks, the doctor fills the canal with gutta-percha - this filling is permanent and periodic refilling is not required.
- Installation of a seal.
But even after placing a permanent filling, the patient still must visit the doctor for an image for another two to three months. It should show a reduction in the size of the existing abscess and restoration of natural tissue.
Endometrioid ovarian cyst (endometrioma)
Cystic endometriosis (endometrioma) is a type of cyst formed by endometrial tissue growing into the ovary. Endometriomas are found in women of reproductive age and can cause long-term bothersome pain in the pelvic area associated with menstruation. Approximately 75% of patients suffering from endometriosis have ovarian damage. On ultrasound, signs of endometrioma can vary, but in most cases (95%) endometrioma appears as a “classic” homogeneous, hypoechoic cystic formation with the presence of diffuse low-level echogenic areas. Rarely, endometrioma is anechoic, resembling a functional ovarian cyst. In addition, endometriomas can be multilocular and contain septa of varying thickness. In approximately one third of patients, careful examination reveals small echogenic lesions adjacent to the wall, which may be due to the presence of cholesterol accumulations, but may also represent blood clots or debris. It is important to distinguish these lesions from true wall nodules; if they are present, the diagnosis of endometrioma becomes extremely likely.
A transvaginal sonogram visualizes a typical endometrioma with hyperechoic foci in the wall. Doppler ultrasound (not shown) failed to detect blood vessels in these lesions.
Endometrioid ovarian cyst: MRI (right) and CT (left). Computed tomography is used primarily to confirm the cystic nature of the formation. MRI can usually be used to better visualize cysts that are poorly differentiated by ultrasound.
On MRI, hemorrhagic contents within the endometrioma lead to increased signal intensity on T1 WI. On T1WI with fat suppression, endometrioma remains hyperintense in contrast to teratomas, which are also hyperintense on T1WI but hypointense on T1FS. This sequence (T1 FS) should always complement MR imaging because it detects small lesions that are T1 hyperintense.
Polycystic ovary syndrome
Radiation diagnostic methods suggest polycystic ovary syndrome (PCOS), also called Stein-Leventhal syndrome, or are used to confirm the diagnosis.
Radiation criteria for PCOS:
- Presence of 10 (or more) simple peripheral cysts
- The characteristic appearance of a “string of pearls”
- Enlarged ovaries (at the same time, in 30% of patients they are not changed in size)
Clinical signs of polycystic ovary syndrome:
- Hirsutism (increased hair growth)
- Obesity
- Fertility disorders
- Acne
- Male pattern hair growth (baldness)
- Or increased androgen levels
What does PCOS look like? On the left, the MRI scan shows a typical “string of pearls” pattern. On the right, in a patient with an increased level of androgens in the blood, an enlarged ovary is visualized, as well as multiple small simple cysts located along the periphery. Obvious is the accompanying obesity. In this patient, MRI can confirm the diagnosis of PCOS.
Diagnostics of education
In order to understand why ovarian cysts appear in women, it is necessary to make a timely diagnosis. You can identify an ovarian cyst at the Yusupov Hospital, where specialists with a high level of qualifications and extensive experience work. A gynecologist can make an assumption about the occurrence of an ovarian cyst even with a routine manual examination on a chair.
To confirm the diagnosis, additional research methods are always prescribed:
- A modern ultrasound machine makes it possible to detect cystic formations early and stop the course of the disease at the very beginning of its occurrence. This helps prevent the development of complications and the appearance of irreversible processes in the organs of the reproductive system;
- Diagnostic laparoscopy is prescribed in especially severe cases, when it is difficult to establish a diagnosis. Several small punctures are made in the abdominal wall, through which a laparoscope, a special optical device, is inserted. This allows you to visualize the patient’s internal genital organs and understand why a cyst appears on the ovary;
- Computed tomography of the ovaries;
- Magnetic resonance imaging;
- Tests to determine the level of sex hormones;
- Tumor markers;
- Puncture of the pouch of Douglas. Used for suspected cyst rupture and internal bleeding.
Most often, if we are not talking about malignant processes, wait-and-see tactics are used in the treatment of ovarian cysts. If a decrease in the diameter of the cyst is not observed, the doctor may prescribe a course of conservative therapy or proceed to surgical treatment.
Make an appointment
Ovarian hyperstimulation syndrome: theca-luteal cysts
Ovarian hyperstimulation syndrome is a relatively rare condition caused by excessive hormonal stimulation of hCG (human chorionic gonadotropin) and usually manifests as bilateral ovarian damage. Excessive hormonal stimulation can occur with gestational trophoblastic disease, PCOS, as well as during treatment with hormones or during pregnancy (rarely in a normal pregnancy with a single fetus) with independent resolution after the birth of the child (according to research results). Excessive hormonal stimulation occurs more often with gestational trophoblastic disease, erythroblastosis fetalosis, or multiple pregnancies. Radiation studies usually reveal bilateral enlargement of the ovaries with the presence of multiple cysts, which can completely replace the ovary. The main differential criterion for ovarian hyperstimulation syndrome is characteristic clinical and anamnestic data.
A sonogram performed on a young pregnant woman reveals multiple cysts in both ovaries. On the right, an invasive formation in the uterus is determined, comparable to gestational trophoblastic disease. The conclusion about this disease was made on the basis of characteristic clinical and anamnestic data (the fact of pregnancy in a young woman) and a sonogram, which revealed signs of an invasive form of gestational trophoblastic disease.
Inflammation of the appendages (salpingoophoritis) and tubo-ovarian abscess
Tubo-ovarian abscess usually occurs as a complication of an ascending (from the vagina to the cervix and fallopian tubes) chlamydial or gonorrheal infection. CT and MRI reveal a complex cystic formation of the ovary with a thick wall and lack of vascularization. Thickening of the endometrium or hydrosalpinx makes the diagnosis of tubo-ovarian abscess more likely.
An axial contrast-enhanced CT scan reveals a complex cystic formation on the left, resembling an abscess, with a thick wall accumulating contrast and gas inclusions inside.
On a CT scan in the sagittal plane (left), it can be seen that the ovarian vein approaches the mass, confirming its nature (arrow). On the coronal tomogram (right), the anatomical relationships of the mass and the uterus can be assessed. A gas bubble is visualized in the uterine cavity, which suggests an infectious onset here, with subsequent spread of infection through the fallopian tube to the ovary.
Main symptoms of an abscess
A dental cyst may not reveal itself for a long time: a person may not realize that there is something wrong with his teeth and gums. Sometimes an abscess causes mild pain when biting or pressing on the gum. But barely noticeable and far from constant pain can force few people to go to the doctor: a cyst at this stage of development is discovered by chance when a person goes to the dentist about completely different teeth.
An infection in the abscess cavity can worsen if immunity decreases: the process of pus formation accelerates, severe pain appears, the cheek swells, the person feels weak and lacks strength, and the temperature rises.
Mature teratoma (dermoid cyst) of the ovary
A mature cystic teratoma, also called a dermoid cyst, is an extremely common ovarian mass that can be cystic in nature. "Mature" in this context means a benign formation as opposed to an "immature", malignant teratoma. Benign cystic teratomas usually occur in young women of childbearing age. On CT, MRI and ultrasound they appear unilocular in (up to) 90% of cases, but can be multilocular or bilateral in approximately 15% of cases. Up to 60% of teratomas may contain calcium inclusions in their structure. The cystic component is represented by a fatty fluid produced by the sebaceous glands located in the tissue lining the cyst. The presence of fat is a diagnostic sign of teratoma. On ultrasound, it has a characteristic cystic appearance with the presence of a hyperechoic solid nodule in the wall, called Rokitansky's node or dermoid plug.
Ultrasound visualizes Rokitansky's node or dermoid plug (arrow).
Liquid-fat levels may also be detected due to density differences (fat, as a lighter, less dense substance, floats on the surface of the water). You can also visualize thin echogenic lines (“stripes”), the presence of which is caused by “hair” in the cyst cavity. Mature cystic teratomas, even benign ones, are most often removed surgically, as they pose an increased risk of ovarian torsion.
Complications of ovarian dermoid cyst:
- Ovarian torsion
- Infection
- Rupture (spontaneous or as a result of trauma)
- Hemolytic anemia (a rare complication that resolves after resection)
- Malignant transformation (rare)
What does an ovarian dermoid cyst look like on an MRI? A cystic formation with hyperintense signal is visible, within which there are septations (found in approximately 10% of such cysts). In the fat suppression mode, the suppression of signal intensity is determined, which makes it possible to confirm the presence of a fatty component and make a conclusion about a teratoma.
Cystadenoma and cystadenofibroma of the ovary
These formations are also common cystic ovarian tumors (cystomas), which can be either serous or mucinous (mucous). On ultrasound, mucinous cystadenoma often appears as an anechoic, unilocular mass that may resemble a simple cyst. Mucinous cystadenomas often consist of several chambers, which may contain complex fluid with inclusions of protein debris or blood. “Papillary” protrusions on the walls suggest a possible malignancy (cystadenocarcinoma).
Ovarian cystoma on ultrasound. Transvaginal examination (top left) reveals a left ovarian cyst measuring 5.1x5.2 cm (anechoic and without septa). However, a nodule is found on the posterior wall of the cyst with no evidence of internal blood flow on Doppler examination (top right); The differential diagnostic range includes a follicular cyst, an accumulation of debris, and a cystic neoplasm. On MRI (below), thin septa accumulating contrast are detected in the formation. No tumor nodes, lymphadenopathy, or peritoneal metastases were detected. The minimum amount of ascitic fluid is determined. The formation was verified as a cystadenoma by biopsy.
Ovarian cystoma: MRI. On MRI scans performed on the same patient five years later, the mass had grown. On T2 WI a complex cyst is visualized in the left ovary with a solid node on the posterior wall. After contrast administration, a slight increase in signal intensity from thin septa and a node in the wall is detected on T1 FS. MRI data did not allow differentiating between benign (eg, cystadenoma) and malignant ovarian neoplasms. Histological examination of the resectate confirmed cystadenofibroma.
Malignant cystic ovarian tumors
Radiation diagnostic methods, such as ultrasound or MRI, are not intended to determine the histological type of tumor. However, with their help it is possible to differentiate benign and malignant neoplasms with varying degrees of certainty and determine further tactics for patient management. Detection of radiation signs of malignant tumor growth should direct the attending physician (gynecologist, oncologist) to further actively determine the nature of the cyst (surgery with biopsy, laparoscopy). In unclear and contradictory cases, it is useful to re-interpret the MRI of the pelvis, as a result of which you can get a second independent opinion from an experienced radiologist.
Get an MRI of the ovaries in St. Petersburg
Complications of a cyst on the root of a tooth
If the cyst was detected too late, complications cannot be ruled out. The following scenarios are possible:
- deformation of the dentition, which is fraught with the installation of removable orthodontic appliances to correct the situation;
- purulent inflammation that develops into abscesses and fistulas;
- pulp destruction;
- damage to healthy teeth;
- blood poisoning and further transfusion.
The only way to avoid complications is timely detection of the disease, so it is extremely important to visit the dentist at least once a year, even if there are no obvious reasons for this.
Serous cystadenocarcinoma
Ultrasound reveals a complex cystic-solid formation in the left ovary, and another large complex formation containing both a solid and a cystic component in the right half of the pelvis
A CT scan of the same patient reveals a complex cystic-solid formation with thickened septa accumulating contrast in the right ovary, extremely suspicious for a malignant tumor. There is also bilateral pelvic lymphadenopathy (arrows). Histopathological examination confirmed serous ovarian cystadenocarcinoma (the most common variant)
CT scan and macroscopic photograph of serous ovarian cystadenocarcinoma.
Ultrasound (left) shows a large multilocular cystic formation in the right parametrium; Some of the chambers are anechoic; in others, uniform low-level echogenic inclusions are visualized, caused by protein content (in this case, mucin, but hemorrhages can also look similar). The partitions in the formation are mostly thin. No blood flow was detected in the septa, the solid component was also absent, and no signs of ascites were detected. Despite the absence of blood flow during Doppler ultrasound and a solid component, the size and multilocular structure of this formation allows us to suspect a cystic tumor and recommend other, more accurate diagnostic methods. Contrast-enhanced CT scan (right) shows similar changes. The formation chambers have different densities, corresponding to different protein contents. Histopathological examination confirmed mucinous cystadenocarcinoma with low malignant potential.
Endometrioid ovarian cancer
Bilateral cystic solid ovarian masses are suspicious for tumor and require further evaluation. The importance of radiological research methods is to confirm the presence of formation; however, it cannot be concluded with absolute certainty that it is benign or malignant. For patients who have epithelial tumors (a much more common group of ovarian neoplasms), even after surgical treatment, determining the exact histological type of the tumor does not affect the prognosis as much as FIGO stage, degree of differentiation, and completeness tumor resection.
The sonogram (left) shows enlargement of both ovaries, inside of which there is both a cystic and soft tissue (solid) component. A CT scan of the same patient reveals a large cystic-solid formation extending from the pelvis to the abdomen. The role of CT in this case is to stage the formation, however, based on CT (MRI) it is impossible to determine the histological structure of the tumor.
Cystic metastases to the ovaries
Most often, metastases to the ovaries, for example, Krukenberg metastases - screenings of stomach or colon cancer, are soft tissue formations, but often they can also be cystic in nature.
A CT scan reveals cystic formations in both ovaries. You can also notice a narrowing of the rectal lumen caused by a cancerous tumor (blue arrow). Cystic metastases of rectal cancer are clearly visible in the recess of the peritoneum (red arrow), which in general are not a typical finding.
Ovarian cancer treatment
Treatment of patients with ovarian cancer has traditionally included initial staging, followed by aggressive cytoreductive surgery in combination with intraperitoneal cisplatin. In early stages (1 and 2), total hysterectomy and bilateral salpingo-oophorectomy are used (or unilateral if a woman of childbearing age wishes to preserve her fertility, although this approach is controversial).
For patients with advanced tumors (stages 3 and 4), cytoreductive intervention is recommended, which involves partial removal of the tumor lesions; This operation is aimed not only at improving the quality of life of patients, but also at reducing the likelihood of intestinal obstruction and eliminating the metabolic effects of the tumor. Optimal cytoreductive intervention involves the removal of all tumor implants larger than 2 cm; with suboptimal, the transverse size of the remaining tumor nodes exceeds 2 cm. Successful cytoreductive surgery increases the effectiveness of chemotherapy and leads to increased survival.
Patients with stage 1a or 1b ovarian tumors may require only elective surgery without subsequent chemotherapy, while more advanced stages require postoperative chemotherapy with cisplatin (the most effective drug for ovarian cancer). Despite the fact that the positive response to platinum therapy reaches 60-80%, about 80-90% of women with the third stage of the disease and about 97% with the fourth stage die within 5 years.
In patients receiving treatment for ovarian cancer, the most effective method of monitoring is measurement of serum CA-125 levels and physical examination. Repeat laparotomy remains the most accurate method for assessing the effectiveness of chemotherapy, but it produces many false-negative results and does not lead to an increase in survival. CT is used to look for a macroscopic lesion and avoids repeat biopsy. If residual tumor tissue is detected using diagnostic methods, the patient may be prescribed additional treatment; however, radiation methods show a large number of false negative results.
Leading specialists in the treatment of cysts and ovarian cysts in the Southern Federal District
Ermolaeva Elvira Kadirovna is a well-known and recognized specialist in the treatment of cysts and ovarian cysts in the North Caucasus. She is a gynecologist, ultrasound doctor, physiotherapist-resortologist. Suffering women and women who want to improve the aesthetics of the genital organs, reduce the size of the vagina and refresh intimate relationships from all regions of Russia and foreign countries.
Ermolaev Oleg Yuryevich Candidate of Medical Sciences, operating gynecologist with 25 years of successful experience in treating cysts and ovarian cysts. Able to see relationships that elude others.
Shchepkin Petr Sergeevich Gynecologist, specialist in the diagnosis and treatment of ovarian cysts and cysts. Experienced ultrasound doctor.
About the doctors of the Clinic in detail...
| INTERNATIONAL RECOGNITION of the reputation and achievements of the Women's Health Resort Clinic in the development and implementation of effective and safe treatment methods and the quality of medical services provided is the AWARDING of the Women's Health Resort Clinic in Pyatigorsk with the SIQS International QUALITY CERTIFICATE in the field of medicine and healthcare. International Socratic Committee, Oxford, UK and Swiss Institute for Quality Standards, Zurich, SWITZERLAND. |
The resort clinic for women's health operates both for paid services and in the voluntary health insurance system.
We work seven days a week and on holidays:
Monday - Friday from 8.00 to 20.00, Saturday, Sunday, holidays from 8.00 to 17.00.
Treatment of cysts and cysts by appointment by multi-line phone 8 (800) 500-52-74 (toll-free within Russia), or +7.
The cost of an initial appointment with a gynecologist is 2,300 rubles.
The cost of a repeated appointment with a gynecologist is 1,250 rubles.
The cost of a pelvic ultrasound is 1550 rubles.
| ONLINE information about the treatment of cysts and ovarian cysts can be found at REGISTER ONLINE for the treatment of cysts and ovarian cysts here. REGISTER online for treatment of ovarian cysts and cysts here. Buy coursework by phone +7 (928) 022-05-32 or here. |
Make an appointment with a gynecologist
The spa clinic for women's health facilitates the accommodation and accommodation of women, women with children and couples during examination and treatment.
Read more about the living conditions and transfer from Mineralnye Vody airport and Pyatigorsk railway station on our website in the article “Accommodation”.
If you need to book accommodation, please coordinate your arrival date no later than 7 days in advance.
We are at your FULL DISPOSAL if you have any doubts or wishes.
- Cost of a planned annual gynecologist examination
- The cost of an appointment with a gynecologist for the purpose of “Checking for EVERYTHING”
- Cost of seeing a specialist to identify breast diseases
- Cost of pelvic ultrasound examination
- Cost of blood tests for cancer markers
Methods for diagnosing the disease
Today, ovarian cysts are quite well diagnosed using a number of tools:
- An examination by a gynecologist, during which the patient’s complaints are clarified, and it is also determined whether the appendages are enlarged and whether there is pain in the lower abdomen.
- Pregnancy test. It is necessary not only to exclude ectopic pregnancy, but also to determine the possibility of performing a computed tomography scan.
- Ultrasound examination, which allows you to quickly and accurately determine the presence of a cyst and monitor the dynamics of its development.
- Laparoscopic examination. Its advantage is that it gives absolutely accurate results and, if necessary, precise and minimally invasive surgery can be performed during the procedure.
- Computed and magnetic resonance tomography.
Choosing a clinic for cyst treatment
A large number of hospitals and dental offices have now opened, but not all of them provide truly high-quality services: situations where people, having parted with money for treatment, not only did not get rid of the disease, but ended up with an even bigger problem, are, unfortunately, not uncommon .
To avoid mistakes, you should try to find out the following information before your visit:
- how long has the dentist been practicing, does he have enough experience to perform surgical interventions;
- The clinic also has dental microscopes in its arsenal, which allow us to examine the affected area in as much detail as possible and efficiently fill the canal.
Choosing a professional doctor is the key to quality treatment the first time.
CT scan for ovarian cyst
CT and MRI are fairly accurate methods that allow you to determine the presence of a cyst, suggest whether it is benign or malignant, clarify its size and exact location, etc. In addition, in the case of a malignant cyst, diagnosis using contrast makes it possible to determine whether the tumor has metastasized to other organs and to accurately determine their location.
CT is performed using X-rays, which makes it possible to obtain sections of the organ in increments of approximately 2 mm. The collected and computer-processed sections are assembled into an accurate three-dimensional image. The procedure is absolutely painless, does not require complex preparation (all you need is to adhere to a certain diet for a couple of days before the procedure and, in case of constipation, take a laxative) and lasts no more than 20 minutes.
Given that the slice step is 2 mm, CT can detect formations of 2 mm in cross section or more. These are fairly small cysts and tumors that are at an early stage of development. Such accuracy of CT diagnostics allows you to begin timely treatment and avoid more serious consequences.
Contraindications to the method are pregnancy (due to exposure of the body to X-ray radiation) and allergic reactions to the contrast agent (in the case of CT with contrast). Such allergic reactions are not very common.
Why does a cyst occur?
The main reason for the development of an abscess is the appearance of infection in the root canals. But there can be several reasons for infection:
- Advanced caries that has developed into pulpitis due to ignoring the need for its treatment. In the tissues on which the carious formation has appeared, pathogenic microorganisms settle, first entering the pulp, as a result of which its inflammation begins, then, if the pulpitis is not treated, penetrating beyond the boundaries of the tooth, resulting in a periodontal abscess.
- Unsatisfactorily filled root canals. Canal filling is a fairly common procedure that dentists have to perform during treatment. However, despite the routine nature of the operation for a dentist, not all specialists, due to lack of experience or due to inattention, carelessness and the desire to complete the work as quickly as possible, do it efficiently. The canal must be sealed along its entire length, since in the unsealed part there is a high probability of infection, which, just as in the case described above, will sooner or later go beyond the boundaries of the tooth and lead to the appearance of an abscess. Official statistics on poorly filled canals are depressing: in more than half of the cases, dentists make mistakes during the procedure, which subsequently result in the appearance of a cyst. In the picture, the unsealed part of the canal is always clearly visible. Sometimes it happens that the root canal is completely filled, but the material used for filling is loose, which is also not good.