Causes of perimaxillary abscess
The causative agents of the disease are representatives of the bacterial flora - streptococci and staphylococci. Factors that can trigger the development of a maxillary abscess include:
- inflammatory processes in the jaw area;
- dental diseases;
- damage to the skin and mucous epithelium in the mouth;
- facial injuries, fractures and dislocations of the jaws;
- infection during dental procedures.
The cause of a maxillary abscess can also be infectious diseases occurring in the form of sepsis.
Opening an abscess, phlegmon of the maxillofacial area
The frequency of development of abscesses and phlegmon of the maxillofacial area of the head is due to the high prevalence of chronic focal odontogenic and tonsillogenic infections, as well as infectious and inflammatory lesions of the skin and oral mucosa. Based on data on the localization of the infectious-inflammatory process in various anatomical sections, zones, regions, as well as spaces of the head and neck, their systematization is built. From the description of the topographic-anatomical structure of the areas of the face, the perimandibular and adjacent areas of the neck, one can see the complexity of their anatomy. There are many cellular spaces, numerous lymph nodes and vessels scattered throughout all areas of the face, an abundant network of arteries and veins with rich innervation of these areas.
The basic principle of treating inflammatory diseases is opening the source of inflammation and draining it. Complete drainage reduces pain, promotes the outflow of wound fluid, improves local microcirculation, which naturally has a beneficial effect on local metabolic processes, the transition of the wound process to the regeneration phase, reducing intoxication and interstitial pressure, limiting the necrosis zone and creating unfavorable conditions for the development of microflora.
The incisional drainage method of treating phlegmons and soft tissue abscesses is quite widespread to this day. It involves opening a purulent focus and open wound management in the postoperative period. The incisional drainage method is a classic one; in general, it determines the tactics for the treatment of acute purulent diseases of soft tissues and purulent wounds.
Opening of the purulent focus is carried out by external access from the skin, or intraoral access from the mucous membrane.
During the operation of opening an abscess (phlegmon), the skin, mucous membrane, and fascial formations above the purulent focus are dissected; the muscles are cut off, peeled off from the place of attachment to the bone of the temporal, medial pterygoid and chewing muscles (m. temporalis, i.e. pterygoideus mcdialis, i.e. masseter) or using a hemostatic clamp, the muscle fibers of the temporal, mylohyoid and buccal muscles (m. temporalis) are pulled apart , T. mylohyoideus, T. buccalis). The exception is the subcutaneous muscle of the neck (m. platysma) and often the mylohyoid muscle, the fibers of which intersect in the transverse direction. which ensures the wound gapes and creates good conditions for the outflow of purulent exudate. Loose tissue located on the way to the purulent focus, in order to avoid damage to the vessels, nerves, and excretory flow of the salivary glands located in it, is stratified and pulled apart with a hemostatic clamp.
Symptoms of perimandibular abscess
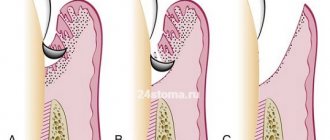
The first sign of the formation of a perimaxillary abscess is toothache, which intensifies when biting in the affected area. Subsequently, the clinical picture of the disease is supplemented by the appearance of edema and the formation of a hyperemic, painful compaction in it. Some patients experience severe facial asymmetry.
Without treatment, the patient's condition worsens. A spontaneous opening of the abscess occurs, the bacterial flora begins to actively multiply in the oral cavity, leading to a chronic process. Chronic suppuration appears from the formed fistula canals, and intoxication of the sick person’s body with decay products is observed.
Oral abscess - symptoms and treatment
Symptoms of oral abscesses are variable and depend directly on the type and location of the abscess. In acute purulent periostitis, patients complain of pain in the area of the causative tooth or jaw segment, swelling of the soft tissues. The face of such a patient is asymmetrical.
When the causative tooth is localized in the frontal part of the upper jaw, the swelling is located in the upper lip and infraorbital region, the nasolabial fold is smoothed. If the diseased tooth is located in the frontal region of the lower jaw, swelling of the soft tissues is noted in the area of the lower lip and chin. When the causative tooth is located in the lateral part of the dentition, perifocal edema (near the infectious focus) is located in the buccal region.
Acute purulent periostitis is usually not accompanied by restrictions in mouth opening. Palpation of regional lymph nodes often reveals signs of acute lymphadenitis (enlarged lymph nodes). When examining the oral cavity, the causative tooth is identified, which usually reacts sharply to tapping (percussion). This is explained by the presence of a pathological process behind the root apex. When examining the vestibule of the oral cavity, a painful inflammatory infiltrate is determined, over which there is an edematous and hyperemic (red) mucous membrane. According to the literature, periostitis is most often located on the side of the cheek or lips, less often on the palatal and lingual side [5][8].
Often abscesses of the maxillo-lingual groove, buccal region, and pterygomaxillary space are considered as a complication of acute purulent periostitis. However, in some cases these diseases develop independently, so there is no reason not to consider them in this review.
Abscess of the maxillo-lingual groove is characterized by a more serious course. The patient complains of pain when swallowing, moving the tongue to the sides, and limited mouth opening. A visual examination reveals swelling of the submandibular area and acute lymphadenitis. Examination of the oral cavity is often difficult and is only possible after blocking the motor branches of the mandibular nerve. When examining the oral cavity, acute or aggravated periodontitis of the chewing tooth of the lower jaw or difficult eruption of the lower wisdom tooth is determined. When examining the maxillo-lingual groove, its bulging is determined; upon palpation, an inflammatory, sharply painful infiltrate can be detected.
With an abscess of the pterygomaxillary space, the patient notes an increase in body temperature, pain in the pharynx, difficulty swallowing, mouth opening is limited, in some cases almost impossible. Visually, perifocal edema is often absent. An examination of the oral cavity can be carried out only after blocking the motor branches of the mandibular nerve. In the oral cavity, difficult eruption of the lower wisdom tooth is usually detected, as well as a hyperemic and edematous pterygomandibular fold.
The clinical picture of an abscess in the buccal region largely depends on the depth of the abscess. With a superficial abscess, hyperemia (redness) of the skin, a local increase in temperature, the skin is tense and does not fold. With a medium and deep location, there is pronounced swelling of the buccal area, the skin is not externally changed, it is difficult to fold into a fold. Local hyperthermia (increased temperature) is usually not observed. When the abscess is deeply located on the mucous membrane of the cheek, marks from teeth are detected.
The condition of patients with these abscesses is usually assessed as moderate. Treatment is usually carried out in a maxillofacial surgery hospital under supervision in order to prevent the development of severe complications. Patients often exhibit symptoms of general intoxication of the body (fever, headaches and muscle pain).
Treatment of maxillary abscess
The main goal of treatment of perimandibular abscesses is the complete elimination of the infectious process and the subsequent restoration of body functions. The main activities aimed at achieving this goal include:
- following a diet with a predominance of purees and pureed soups;
- opening the abscess and draining the resulting cavity;
- antibacterial therapy;
- vitamin therapy;
- taking immunostimulants;
- detoxification therapy;
- taking analgesics;
- rinsing the mouth with solutions of furatsilin and soda.
With timely and professional treatment, the prognosis of the disease is almost always favorable. Full recovery of the patient occurs after 1.5 - 2 weeks from the date of the start of treatment in the department of dental surgery at Adent.
Diagnosis of the disease
Establishing a diagnosis for acute odontogenic infections includes the following measures:
Collection of medical history. The doctor finds out the patient’s complaints and the general condition of the patient. External examination of the maxillofacial area and palpation of regional lymph nodes. Most inflammatory and purulent processes cause enlargement and pain of the lymph nodes. Instrumental examination of the oral cavity, during which the doctor detects chronic foci of odontogenic infection. X-ray in frontal and lateral projection. Laboratory blood test, in which there is an increase in SOE, leukocytes and a decrease in the concentration of red blood cells and hemoglobin.
Complications of abscesses and phlegmon
Purulent lesions of the maxillofacial area can be complicated by the following pathologies:
Sepsis is a serious condition of the body that is caused by the penetration of a bacterial infection into the circulatory system. Treatment of such a complication is difficult due to the development of body resistance to antibiotic therapy. Sepsis is often the cause of death. Mediastenitis in the form of purulent inflammation of the tissue of the mediastinum, where the heart, lungs and bronchi are located. Meningitis . Inflammatory damage to the meninges develops as a result of the spread of purulent infection through the lymphatic and blood vessels of the head.
General principles of treatment of the disease
The doctor who treats phlegmon of the maxillofacial area is an oral and maxillofacial surgeon.
Each doctor, when starting to treat an odontogenic process in the maxillofacial area, is guided in his actions by the following principles:
The tooth that caused the development of phlegmon is removed. Timely diagnosis is very important due to the characteristics of this area, from where the infection can spread, causing severe consequences (in particular, mediastinitis). It is necessary to eliminate the spread of the infection, that is, promptly open the lesion and eliminate the inflammatory exudate, relieve tissue tension. The rate of subsidence of inflammation depends on the quality of evacuation of all decay products from the wound, that is, careful postoperative treatment of the wound is necessary. Comprehensive treatment of pathology using all means and methods available in this medical institution. Friendly management of the patient with colleagues from other areas, timely appointment of consultations with all specialists for combined lesions. Visible external changes often occur, which are not always pleasant for the patient, which is especially painful in the face area. Therefore, there is an urgent need to organize work with patients by a medical psychologist in the early stages after surgery, especially if there is a significant visible defect. Correct stage-by-stage treatment, organization of medical rehabilitation, referral to the appropriate department with complete information about the patient. Fully informing relatives and the patient about the violation of significant functions of the maxillofacial area, if any. Upon leaving the hospital, the patient should have clear further recommendations, especially if it is necessary to continue treatment on an outpatient basis.
Forecast and prevention of the disease
The prognosis of odontogenic abscesses and phlegmons is usually favorable. A positive treatment result is observed with timely indication of full surgical care. In such cases, the patient must be hospitalized in a specialized medical hospital.
Lethal outcomes from purulent lesions of the soft tissues of the maxillofacial area are associated with late presentation of the patient and systemic suppression of his immunity.
Prevention of the disease is achieved in the following ways:
sanitation of the oral cavity, during which the dentist treats all carious, pulpitic and periodontitis teeth; strict adherence by patients to the rules of personal hygiene and regular brushing of teeth; undergoing regular preventive examinations at the dentist, at least twice a year; timely consultation with a doctor if symptoms of dental diseases are detected. Every person should remember that the cost of prevention is much lower than the cost of treatment. And in some cases, sanitation of the oral cavity can prevent the development of severe complications, which are accompanied by high mortality in patients.