Causes of inflammation
Most inflammatory diseases of the maxillofacial area are associated with dental pathology. These include periostitis, osteomyelitis , lymphadenitis and others. As a rule, they arise as a result of various dental diseases or tissues surrounding the teeth. In addition, the causative agents of inflammatory infections can be staphylococci, streptococci, candida fungus and other microorganisms, including those that are present in the oral cavity of every person. Often, infection occurs due to defects in the surfaces of teeth: carious lesions. This becomes an entry point for infection. Complications are associated with the fact that tooth tissue is not able to recover naturally. Therefore, the longer you wait to go to the dentist, the higher the risk of developing inflammation.
Classification of the disease
Depending on the origin, necrosis of the jaw can be of the following types:
- odontogenic (develops as a result of dental disease);
- hematogenous (associated with the spread of infection through the bloodstream);
- traumatic (occurs as a result of direct trauma to the jaw).
According to the nature of the course, osteonecrosis can be acute, subacute or chronic. In most cases, it is preceded by dental disorders, including the formation of fistulas and gumboils.
Depending on the intensity of clinical manifestations, necrosis of the jaw can have several degrees of development:
- 1st degree: bone tissue is destroyed by 10%, while the functional abilities of the jaw are not impaired;
- 2nd degree: microcracks occur, severe pain appears, and restrictions in the movements of the maxillofacial area appear;
- 3rd degree: more than 50% of tissues are affected, pain is expressed, which is permanent;
- Grade 4: massive bone destruction requires urgent surgical intervention.
It is recommended to seek medical help at the initial stage of the disease, when it is possible to avoid traumatic operations and completely restore impaired functions.
Symptoms of jaw necrosis
The severity of clinical manifestations of jaw necrosis depends on the state of immunity and the severity of the disease. If the disease is preceded by acute osteomyelitis, then the body temperature rises sharply, chills, severe weakness and weakness, and sleep disturbance appear.
Additional signs of osteonecrosis of the jaw:
- pain in the area where the infected tooth is located, which intensifies with pressure;
- pathological mobility of teeth;
- swelling of the mucous membrane;
- the appearance of purulent discharge from the gum pockets;
- bad breath;
- enlargement of regional lymph nodes;
- when the focus of infiltration spreads, restrictions appear when opening the mouth, pain occurs during swallowing, and breathing may be impaired;
- decreased sensitivity of the soft tissues of the affected jaw, feeling of numbness and tingling;
- asymmetry of facial contours.
The main symptom of the disease is pain in the area of the affected tooth, which is the main source of infection. The pain syndrome tends to intensify, radiating to the area of the eyes, ear and head.
Over time, the diseased tooth becomes mobile, and pus begins to ooze from the gums. These alarming signs should force you to contact your dentist as soon as possible and undergo an appropriate examination.
Necrosis can have a subacute course, when there are no obvious signs of an acute infectious inflammatory process. In this case, the general condition of the patient may improve, suppuration disappears, but the mobility of the affected teeth increases.
In the destructive form of the disease, signs of intoxication predominate, and there is a significant enlargement of the lymph nodes located in the submandibular zone. Fistulas with purulent exudate may form. The chronic course of osteonecrosis is often the cause of a pathological fracture of the jaw, the formation of small sequesters and infiltrates.
A doctor can detect jaw necrosis based on the characteristic symptoms of the disease and changes in laboratory diagnostic parameters. The presence of infection is confirmed by an increase in the number of leukocytes and an increase in ESR in a general blood test. To assess the degree of damage to bone tissue and detect the exact location of the infection, X-ray examination methods are required.
Survey
In some people, necrosis of the jaw occurs for a long time without significant symptoms. The disease is often discovered by chance during a routine examination or examination.
Main diagnostic methods:
- radiography;
- biochemical blood test, general blood and urine analysis;
- bacteriological culture of discharge from a purulent focus.
On a hemogram with necrosis of the jaw, specialists detect neutrophilic leukocytosis, eosinopenia, and an increase in ESR. Based on the results of a biochemical blood test, one can suspect the development of the disease due to a large amount of C-reactive protein and hyperglobulinemia. Red blood cells, protein substances and casts are found in the urine.
Based on the results of X-ray or tomography of the jaw, it is possible to identify foci of sequestration, areas with coarse fibrous bone tissue, areas of osteosclerosis and uneven contours.
Necrosis requires differential diagnosis with osteomyelitis, periodontitis, periostitis, purulent cysts and tumors of the jaw. The effectiveness of the chosen treatment depends on the accuracy of the diagnosis.
Features of treatment
If you seek dental care in a timely manner, the prognosis for osteonecrosis of the jaw is favorable. It is important to determine the root cause of the disease in order to stop the action of infectious pathogens.
The dental surgeon must eliminate the primary purulent focus. In the case of an odontogenic form of the disease, it is necessary to remove the tooth; in a hematogenous form, it is necessary to sanitation the infection; in a traumatic form, primary surgical treatment of the wound must be performed.
Main measures for necrosis of the jaw:
- Opening any purulent formations, antiseptic treatment and prescribing antibiotics after an individual sensitivity test.
- Prescription of painkillers, anti-inflammatory drugs, agents that accelerate tissue regeneration.
- Detoxification measures include the prescription of medications that help remove poisons and toxic compounds from the body.
- Periostotomy is prescribed, pus is evacuated and bone tissue is washed with antiseptic solutions.
- After removing dead tissue, the dentist can strengthen the teeth with therapeutic splinting.
- Additionally, hyperbaric oxygenation, ultraviolet blood irradiation, plasmapheresis, and local physiotherapy, including the use of ultrasound and UHF, are prescribed.
- Chronic necrosis is an indication for removal of sequestered bone tissue fragments. After this, an antiseptic rinse is carried out and the bone is filled with special materials with antibiotics.
Treatment of necrosis is long and quite complex. It requires the use of specific medications. Therefore, it is not recommended to carry out therapeutic measures at home. Of the traditional methods, only decoctions and infusions of anti-inflammatory herbs can be used as a supplement to the main drug therapy.
Often necrosis of the jaw develops against the background of oncological lesions of the maxillofacial area. This requires additional consultation and collaboration between the dentist and the oncologist. In this case, surgical interventions cannot be avoided. But you shouldn’t waste time thinking and self-medicating.
Prognosis and prevention
Acute infectious lesions of bone tissue are always dangerous. But with timely treatment, severe complications can be avoided. If the course is unfavorable, the disease is complicated by meningitis, abscess of the brain, lung, sepsis and mediastinitis. Chronic osteonecrosis often ends in ankylosis of the TMJ, contractures, and pathological fractures of the jaw.
It is important to pay increased attention to the quality of oral care, regularly visit the dentist and, when the first signs of the disease appear, undergo comprehensive treatment.
Only a doctor can monitor the condition of the gums and teeth, detect the first signs of problems and take everything necessary to prevent secondary infection. To get a consultation
Types of inflammatory diseases of the maxillofacial area
At the MedicPro clinic, an oral and maxillofacial surgeon in Kaluga treats all types of inflammation in the face and oral cavity. An important component of treatment is eliminating the cause of the inflammatory process. Without this, any therapy will be ineffective and will only provide temporary relief.
Lymphadenitis
This disease is inflammation of the lymph nodes. They perform an important function: they prevent the spread of infections from the lesion. Most often, submandibular (cervical) lymphadenitis occurs in adults: treatment of this disease is aimed at eliminating the inflammatory process and the source of its occurrence. There are nonspecific and specific lymphadenitis, which can be caused by various reasons. In the first case, purulent wounds, advanced stages of caries, boils, and phlegnomas become the source of inflammation. The second type is caused by various infections. In addition, there are purulent and non-purulent forms of lymphadenitis in an adult on the neck: treatment is selected in accordance with the indications. The factors that caused the disease, as well as symptoms, are taken into account. The disease can occur in chronic and acute forms. In order to prevent development into chronic lymphadenitis, it is important to begin treatment as soon as the first signs of this pathology appear:
- pain in the area of the lymph nodes (under the jaw);
- increase in size of lymph nodes;
- increased body temperature;
- redness of the skin in the area of the lymph nodes;
- pain when chewing and swallowing;
- general weakness and fatigue;
- loss of appetite.
Despite the fact that there are more than 600 lymph nodes in the human body, lymphadenitis in the neck and axilla is most often sought for treatment . Inflammatory processes in the inguinal lymph nodes are also common. At the MedicPro clinic we treat cervical lymphadenitis at any stage. A thorough diagnosis is carried out in advance. It is important to differentiate the disease from oncology and leukemia.
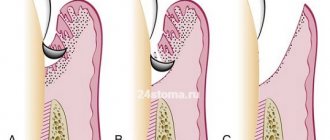
Periostitis
An inflammatory disease of the periosteum caused by pathogenic microorganisms. They penetrate through lesions of the teeth and gums. The most common causes of periostitis of the jaw are chronic periodontitis, periodontitis with complications, other inflammatory processes, as well as advanced dental caries. The disease periostitis has characteristic symptoms:
- swelling above the gum at the site of the lesion;
- the presence of a source of infection - a diseased tooth with signs of an inflammatory process;
- pain spreading from the site of the lesion to the neck, eye, temple;
- increased pain when pressing on the tooth at the site of the infection;
- increased body temperature;
- general weakness of the body, loss of appetite;
- swelling of the cheek due to inflammation;
- restriction of jaw movement.
Diagnosing gum periostitis is simple by examining the patient and taking a medical history. Additionally, radiography may be prescribed to determine the depth of the inflammatory process. For the treatment of periostitis of the upper and lower jaw , the most appropriate treatment is selected:
- Conservative - in the early stages, during the acute course of the disease, without the formation of a purulent sac. The patient is prescribed antibiotics, anti-inflammatory and painkillers, physiotherapy, and dental sanitation. The decision to remove a tooth that has become a source of infection is made individually by the doctor.
- Surgical - used to treat progressive periodontitis of the tooth if conservative treatment has failed. The site of inflammation is excised, accumulations of pus are eliminated. Most often, the tooth is removed.
In order to exclude complications and the transition of the disease to chronic periodontitis , it is important to consult a doctor in a timely manner.
Osteomyelitis
The disease develops due to the penetration of pathogenic bacteria into the bone tissue of the jaw and periosteum. The bone marrow is also often affected. There are acute forms of the disease, as well as chronic osteomyelitis of the jaw: treatment is selected in accordance with the indications individually for each patient. There are two ways for bacteria to penetrate the lesion: from the outside (exogenous osteomyelitis) and through the bloodstream (endogenous). The first is the most common and occurs as a result of injury or from the inflammatory process of surrounding tissues. The second most often occurs in childhood. The disease is accompanied by general malaise, up to a serious condition, with signs of intoxication. There is swelling at the site of the lesion, pain that increases with pressure, and redness of the skin. The temperature rises. If osteomyelitis is not treated , these symptoms intensify and the patient's condition worsens significantly. Intensive therapy with antibiotics and anti-inflammatory drugs is used to treat osteomyelitis Often the acute form requires the installation of drainage to eliminate pus. To do this, a burr hole is made, through which the lesion is also washed with an antibiotic solution. Surgical treatment is required only in complex cases, with the appearance of purulent fistulas, sequestration, or at the chronic stage with signs of intoxication. In this case, the affected tissue is removed and the bone is restored using plastic surgery. Moreover, the price of treatment for osteomyelitis directly depends on the complexity.
Abscess
Acute inflammation that can be localized in various tissues in the oral cavity. Most often, gum and tooth abscess , which occurs due to insufficiently thorough hygiene. Bacteria penetrate through defects in the tooth surface or gum tissue and subsequently provoke purulent inflammation. An abscess of the maxillo-lingual groove, floor of the mouth, hard palate or cheek also develops due to bacteria entering an open wound. In the absence of timely treatment, it progresses quickly. The disease occurs with severe symptoms:
- pain at the site of the lesion ( a tooth abscess is characterized by pain when pressing on the tooth or gum itself);
- swelling that increases over time;
- increased body temperature;
- headaches, severe weakness;
- the appearance of bad breath and bitter taste;
- facial asymmetry appears externally;
- pain and discomfort while eating;
- enlarged cervical lymph nodes.
treatment of an abscess of a tooth, jaw, gum , and other tissues as quickly as possible. Advanced inflammation can provoke complications in the form of intoxication of the body and spread of the inflammatory process to other tissues (including bone). The patient is prescribed anti-inflammatory drugs and antibiotics. Tissue cleaning is also carried out to eliminate purulent accumulations. In the case of a tooth abscess, complications may lead to removal. This treatment is taken by the doctor depending on the picture of the disease.
The problem of treating purulent-inflammatory diseases (PIDs) of the face and neck is relevant for both dentists in clinics and maxillofacial surgeons in hospitals. About 50% of people in maxillofacial hospitals, and about 20% who seek help from a dentist and surgeon in polyclinics, are patients with inflammatory diseases of the maxillofacial area (MFA), among them 60–80% of patients with abscesses and phlegmon, the incidence of which has increased 1.5–2.0 times over the last decade [1–3]. There has been a steady increase in atypically and severely progressing phlegmons, spreading simultaneously in several cellular spaces, with the development of such serious complications as sepsis, contact mediastenitis, thrombosis of the cavernous sinus of the dura mater [4–9]. Low-symptomatic “erased” forms of phlegmon occur among 13.4–22% of patients, are characterized by a long course and present difficulties for diagnosis, which contributes to late hospitalization and untimely treatment [10–12]. The microbial etiology of maxillary sinusitis is determined by the localization of the primary process (connection with the oral cavity, teeth) [13, 14].
As a rule, there are associations of 2–6 types of microorganisms: aerobes (streptococci and staphylococci) and obligate anaerobes (bacteroides, fusobacteria, peptococci, peptostreptococci) [15, 16]. The frequency of isolation of anaerobes is up to 52–68%, less often in non-odontogenic processes of the maxillofacial lesion – 20%, in odontogenic processes – 67.7–96% [13, 15–18].
Being in symbiosis, bacteria gradually enter into antagonistic and synergistic relationships during the development of infection. This explains the negative dynamics of the clinical picture of the disease in mixed anaerobic-aerobic infections. For example, it was noted that representatives of the genus Veillonella exhibit weak pathogenicity in monoculture, and the synergistic effect of accompanying aerobic microbes increases the pathogenicity of these bacteria. Purulent-inflammatory processes occurring with the participation of associations consisting of pepto-, peptostreptococci and gram-positive cocci are more severe and more extensive than lesions caused by a monoculture of aerobic gram-positive cocci [19].
The main causative agents of gastrointestinal infections of the maxillofacial area
GVZ of the maxillofacial area and neck, requiring surgical intervention, are often of odontogenic origin and are complications of an infectious process in the oral cavity. The spread of inflammation is possible by contact - through fascial spaces (infection of the floor of the mouth) and hematogenous.
Oral infections are divided into the following types depending on the anatomical location [1]:
- odontogenic, associated with damage to tooth tissue (caries, pulpitis);
- periodontal, including periodontium (periodontitis) and gums (gingivitis, pericoronitis), surrounding soft and bone tissue.
The main causative agents of odontogenic infections are microorganisms that are constantly present in the oral cavity: mainly viridans streptococci (Streptococcus mutans, Streptococcus milleri), non-spore-forming anaerobes (Peptostreptococcus spp., Fusobacterium spp., Actinomyces spp.). In case of periodontal infection, five main pathogens are most often identified: Porphyromonas gingivalis, Prevotella intermedia, Eikenellacorrodens, Fusobacterium nucleatum, Aggregatibacter actinomycetemcomitans, and less commonly – Capnocytophaga spp. [20, 21]. Depending on the location and severity of the infection, the patient’s age and concomitant pathology, changes in the microbial spectrum of pathogens are possible.
Thus, severe purulent lesions are associated with facultative gram-negative flora (Enterobacteriaceaeespp.) and Staphylococcusaureus. In patients with diabetes mellitus, elderly people and patients hospitalized in a hospital, Enterobacteriaceae spp. also predominate. [22].
Research by Yu.V. Alekseeva (2005) demonstrated that Staphylococcus spp. is isolated in odontogenic inflammatory diseases. (15%), Streptococcus spp. (6%) and obligate anaerobic bacteria (79%). Anaerobes are represented by gram-positive microorganisms - Bacteroides spp., Fusobacterium spp., gram-positive cocci. In 86%, resident flora is sown, in 7%, pathogenic strains are sown.
In studies by L. Chavez de Paz, G. Svensater, G. Dalen, G. Bergenholtz (2004), it was found that Streptococcus gordonii, Streptococcus anginosus, Streptococcusoralis, and Enterococcus spp. were most often isolated from the root canals of teeth with chronic destructive periodontitis. Lactobacillus paracasei.
The development of odontogenic periostitis and osteomyelitis in 50% of cases is caused by S. aureus and Streptococcus spp., but, as a rule, anaerobic flora prevails: Peptococcus niger, Peptostreptococcus spp., Bacteroides spp. [25].
In non-odontogenic osteomyelitis, the key pathogens are methicillin-sensitive staphylococci (MSSA) - 52%, coagulase-negative staphylococci (CNS) - 14%, methicillin-resistant staphylococci (MRSA) - 2% and Pseudomonas aeruginosa (4.4%) [26]. Traumatic osteomyelitis is often caused by the presence of S. aureus, as well as Enterobacteriaceae spp., P. aeruginosa [27].
The causative agents of odontogenic maxillary sinusitis are non-spore-forming anaerobes - Peptostreptococcus spp., Bacteroidesspp., as well as Haemophilus influenzae, Streptococcus intermedius, Streptococcus pneumoniae, Moraxellacatarrhalis, Streptococcus pyogenes. Isolation of S. aureus from the sinus is characteristic of nosocomial sinusitis [22].
Purulent odontogenic infection of the soft tissues of the face and neck is associated with the release of polymicrobial flora: Streptococcus spp., Staphylococcus spp., Peptostreptococcus spp., Bacteroidesspp., F. nucleatum, Enterobacteriaceaespp., Veillonellaspp., Eikenellaspp. The causative agents of abscesses and phlegmon of non-odontogenic origin, most often caused by skin damage, are S. aureus, S. pyogenes. In 50.9% of patients with phlegmon of the face and neck, anaerobic bacteria Peptostreptococcus spp., Bacteroides spp., Veillonellaspp. are isolated; Staphylococcus spp. – in 23.7% of observations, Streptococcus spp. – in 18.6% [28].
For putrefactive-necrotic phlegmon of the face and neck, a polymicrobial flora is isolated, including F. nucleatum, Bacteroidesspp., Peptostreptococcus spp., Streptococcus spp., Actinomycesspp. In addition to the microorganisms mentioned above, gram-negative bacteria and S. aureus are often isolated from patients with severe disease [25]. Klebsiella spp., Enterococcus spp., S. aureus, P. aeruginosa play an important role in patients with diabetes mellitus, and the presence of P. aeruginosa is associated with the most unfavorable prognosis [29, 30].
When lymphadenitis of the face and neck develops, group A β-hemolytic streptococcus and S. aureus are isolated in 70–80% of cases. Anaerobic pathogens, such as Bacteroides spp., Peptostreptococcus spp., Peptococcus spp., F. nucleatum, Propionibacterium acnes, can cause the development of odontogenic lymphadenitis [22].
Principles of empirical antibacterial therapy (ABT) and features of the use of antibiotics in dentistry
Treatment of patients with maxillofacial infarction is complex and includes surgery, local treatment of a purulent wound, systemic ABT, physical therapy, and, if indicated, detoxification and immunocorrective therapy. The tactics of surgical treatment have now been defined quite fully. It includes the opening of a purulent-inflammatory focus by layer-by-layer dissection of the tissue above it, as well as drainage of the surgical wound in order to create conditions for the evacuation of purulent exudate containing pathogens, their metabolic products and tissue breakdown [3, 31].
According to Medical Advertising News (USA), dentists prescribe from 2 to 10 antibiotics daily, antibiotics are especially often used by patients with complaints of pain and swelling of the soft tissues of the face [32]. There is virtually no data confirming the advisability of systemic ABT for many procedures in dentistry. Moreover, the results of randomized clinical trials indicate the undesirability of systemic use of antibiotics in outpatient practice [33]. The oral cavity, in a figurative expression, is the “cradle of resistance”, since it abounds in flora, the etiological significance of which in the development of the source of infection is often not identified, and inadequate use of antimicrobial drugs changes the qualitative response of not only clinically significant pathogens, but also representatives of obligate, as well as facultative flora. ABT is often carried out in a hospital without bacteriological control, which contributes to the development of microflora resistance, allergization of the body, and disruption of intestinal microbiocenosis [34, 8, 35].
In the clinic of surgical dentistry, antibiotics are used for intravenous lesions of the maxillofacial area and for the purpose of prevention (for injuries of soft tissues and bones of the face, after implantation, reconstructive operations, systemic prophylaxis with artificial heart valves) [33].
When planning empirical ABT, it is necessary to focus on individual fluctuations in the qualitative and quantitative composition of the oral microflora, which depend on age, diet, hygiene skills, and the presence of pathological processes in the teeth and gums. The rational choice of antibiotics is facilitated by the use of rapid methods for determining the sensitivity of identified pathogens to them, focusing on the most clinically significant of these drugs, and assessing the organoleptic properties of wound exudate [36, 37]. When thick, creamy pus is obtained from the lesion, it can be assumed that the causative agent is staphylococcal flora; when receiving liquid, foul-smelling pus - a microbial association with a predominance of gram-negative bacillary flora. If pus is not obtained from the wound, but a cloudy-reddish liquid is released, the presence of anaerobic microflora can be assumed [22].
When planning treatment in a dental clinic, it is advisable to focus on oral antibiotics with high bioavailability, a long half-life, and minimal impact on the intestinal microflora [38]. When treating a patient in a hospital setting, it is advisable to choose a drug that has forms for parenteral and oral administration for the purpose of stepwise therapy [39].
At the outpatient stage, ABT is carried out for acute and exacerbations of chronic periodontitis, acute periostitis, purulent-inflammatory diseases of the soft tissues of the maxillofacial area, i.e. processes that tend to spread. For prophylactic purposes, antibiotics are used during surgical interventions (removal of impacted and dystopic teeth, cystectomy, tooth-preserving operations, implantation) [40].
The main reasons for the ineffectiveness of ABT may be:
- undrained focus of purulent inflammation or the presence of a foreign body in the wound;
- non-bacterial pathogen of an infectious process (viruses, fungi);
- inadequate choice of antibiotic (the pathogen is naturally resistant);
- changes in the sensitivity of the pathogen during treatment;
- use of subtherapeutic doses of the drug, violation of the method of administration or administration technique (violation of instructions for dilution and storage);
- purulent-inflammatory processes of the maxillofacial area are a complication of the underlying disease (congenital cysts, neoplasms);
- superinfection with hospital microflora.
Antibacterial drugs recommended for the treatment of patients with gastrointestinal tract infections of the face and neck are presented in the relevant regulatory documents of the Ministry of Health and Social Development of the Russian Federation. When treating abscesses, boils, carbuncles of the soft tissues of the maxillofacial area, cephalosporins (cefuroxime) or macrolides (erythromycin) are recommended - order No. 126 of 02/11/2005, for phlegmons - cefuroxime, amoxicillin/clavulanate, spiramycin, levofloxacin - order No. 477 of 07/29/2005, for osteomyelitis - pefloxacin, levofloxacin, ceftazidime, cefuroxime, imipenem, rifampicin, ceftriaxone - order No. 520 of 08/11/2005.
Currently, we do not have fundamental recommendations for ABT for intravenous thromboembolism. At the same time, the resistance status of oral microflora (S. aureus, S. pyogenes, viridans streptococci, gram-negative microorganisms and even Candida fungi) has changed significantly. Among the initially present resistant strains, during selection, associated polyresistance to the most commonly used antibiotics (macrolides, penicillins) appeared. Of particular concern are cases of nosocomial infection of the maxillofacial area, accompanied by a systemic inflammatory response, spread of the process to vital areas (mediastinum, cranial cavity), and unfavorable outcome. Vancomycin and linezolid should be used in initial therapy if there is a risk of isolating MRSA strains, and risk factors for isolating extended-spectrum β-lactamase producers (Enterobacteriaceae spp.) are the basis for prescribing carbapenems. The prospects for the optimal choice of antimicrobial drug for Pseudomonas aeruginosa infection, unfortunately, are not clear today.
In clinical practice, dental surgeons widely use antibiotics for prophylactic purposes in the treatment of facial bone fractures. There is evidence of the advisability of prophylaxis during primary surgical treatment, however, continuing the course of ABT after repositioning of fragments does not reduce the overall incidence of infectious complications [41].
.The main pathogens of HVO of the maxillofacial area.
Dental manipulations in the oral cavity can lead to hematogenous spread of microorganisms (or their metabolic products, or immune complexes) with the development of distant sites of infection [42]. The questions of when and under what circumstances antibiotic prophylaxis is required for diseases of the maxillofacial area remain controversial [43].
Thus, rational ABT and antibiotic prophylaxis in dental practice are one of the mechanisms regulating the state of resistance in general. Limiting the systemic use of antibiotics in outpatient dentistry, reducing ABT courses and de-escalation therapy with adequately selected antimicrobial drugs for severe and nosocomial infections of the maxillofacial area is the main way to improve the quality of care for patients with intravenous infections of the maxillofacial area and neck.
Information about the authors: Kovaleva Natalya Sergeevna – assistant at the Department of Surgical Dentistry, SGMA; Antonina Petrovna Zuzova – Candidate of Medical Sciences, Associate Professor of the Department of Clinical Pharmacology, SSMA. Email
Treatment of inflammatory diseases in Kaluga
If any symptoms of the above diseases occur, it is important to consult a doctor immediately. Even a day of delay can result in serious complications. An oral and maxillofacial surgeon working in our clinic will conduct a thorough examination and prescribe competent treatment. Make an appointment by phone or through the feedback form on the website.
We are always happy to help you and invite you to medical assistance! Be alert! You can make an appointment by phone; 8 (4842) 27-72-50.