Root canal treatment is a necessary procedure to save and restore the affected tooth. It is necessary to completely clean the root canal of pathogenic microorganisms and necrotic tissue, and also seal it with filling material. At the Implantmaster clinic, tooth canal treatment is carried out under a microscope, which improves the quality of treatment and makes filling more reliable. If the inflammation at the root is not treated in time, it will develop deeper and it will be very difficult to save the tooth.
Complicated forms of dental caries (pulpitis and periodontitis), affecting the canals in the teeth, make up about one third of the structure of dental diseases and require complex endodontic manipulations by a dentist. Symptoms, such as sharp pain in the affected tooth, reaction to temperature stimuli, pain when biting, are familiar to most people. If the dentist has the necessary knowledge and skills, patients can count on quality treatment.
Issues regarding endodontic intervention are still relevant. New trends in endodontics require improving the knowledge and skills of doctors. In the innovative dental clinic “Implantmaster” in Moscow, dental canal treatment is carried out with the participation of highly qualified specialists who regularly improve their skills in the best clinics in Europe, as well as by watching webinars of leading specialists, participating in scientific conferences and symposiums. We are accustomed to solving complex problems in the shortest possible time and satisfying the needs of even the most demanding patients. Our doctors work with advanced materials, use modern equipment for the treatment of dental canals, setting loyal prices for the services provided.
Next, we will talk about the features of tooth canal treatment and what diseases require its use. You will also learn about the main stages of the treatment method and the nuances of treatment using a microscope. You will be able to familiarize yourself with the possible complications after treatment. You will learn about this and much more about root canal treatment below.
What is a root canal?
In the oral cavity, each tooth, in addition to the hard tissues of the crown, also has soft tissues - the pulp chamber, which communicates with thin tubes running along the entire root - root canals. All functional groups of teeth have a different number of roots, and therefore canals. The front group of teeth has one canal, the lateral group has 2-4. At the apex of the root there is an apical foramen, which is the entrance window to the canal. Vessels and a nerve pass through it into each root canal, which are responsible for the flow of blood and tooth sensitivity.
Endodontic treatment is a procedure for removing the affected, inflamed or dead neurovascular bundle, with further mechanical and medicinal treatment of the resulting space, as well as dense filling of the root canals with a special material.
Features of the structure of the roots of temporary teeth
In almost every case of treatment, the dentist can observe various deviations from the standard norms of topographic anatomy. However, the greatest number of differences occurs between temporary and permanent teeth. The most common and well-studied features are the following:
- small size of roots and crowns;
- a noticeable difference in the diameters of the chewing surface and the equator;
- wide arrangement of canals at molars;
- smaller ratio of root length to crown height;
- increased volume of the intradental cavity;
- distal deviation of the root apices of the anterior teeth;
- small thickness of hard tissues (enamel, primary dentin);
- the minimum distance between the mesial and other pulp horns;
- large width of cone-shaped channels;
- dynamic change in root topography due to the formation of secondary dentin;
- strong connection between the periodontium and the pulp using “mixed tissue”;
- plasticity and a higher degree of protection against resorption;
- maintaining the normal functioning of the nervous network when 1/3 of the root is damaged;
- constant change in the apical part due to active development or resorption.
Principle of dental canal treatment
The specific shape and function of each tooth in the jaw determines the mechanics of treatment. Endodontic treatment of canals in teeth of various functional groups has its own subtleties.
Canal treatment in the frontal group of teeth.
The teeth of the frontal group are mostly single-channel. The canals are tortuous and difficult to clean instrumentally. To maintain aesthetics, the cavity is opened from the lingual side; it is also important to preserve the color of the tooth enamel, which is why filling materials without dyes are used.
Treatment of canals in wisdom teeth.
“Eights” may have more than five canals with a branched structure, which is not always visible on a targeted X-ray. These conditions, coupled with their difficult-to-reach location, make proper root canal treatment difficult. At the end of the canal treatment procedure, filling pastes are used. For more accurate diagnostic data, at our innovative dentistry “Implantmaster” in Moscow, when treating canals, in addition to the ability to take a panoramic image of the teeth and a targeted X-ray image, we have a new type of CT scan - Cone-beam computed tomogram. The pictures are more accurate, and the X-ray radiation is even less.
Root canal treatment in temporary teeth.
The canals in the temporary dentition are treated endodontically at the stage when the root is stable. When choosing actions when treating tooth canals, their structure is taken into account: the thin structure of the canal itself, low saturation of dentin with microelements and a wide apex. For filling, zinc oxide eugenol and iodoform pastes, materials containing calcium hydroxide, are used. These materials do not affect the permanent tooth germ, dissolving together with the root of the temporary tooth.
Our team of doctors
Maxillofacial surgeon, Implantologist
Bocharov Maxim Viktorovich
Experience: 11 years
Orthopedist, Neuromuscular dentist
Stepanov Andrey Vasilievich
Experience: 22 years
Endodontist, Therapist
Skalet Yana Alexandrovna
Experience: 22 years
Orthopedic dentist
Tsoi Sergey Konstantinovich
Experience: 19 years
Endodontist, Therapist, Orthopedist
Varvyanskaya Anastasia Andreevna
Experience: 6 years
Dentist-orthodontist
Enikeeva Anna Stanislavovna
Experience: 3 years
Indications for endodontic therapy
Treatment of tooth canals is carried out according to precise indications, because as a result of manipulations, the tooth is deprived of the vessels and nerve that feed it. Dental tissue becomes less durable and more fragile. Indications are: subjective data, results of an objective examination of the patient in a chair, radiography (CBCT, OPTG and targeted X-ray), inflammation and infections that accompany the destruction of hard tissues and trauma.
- Pulpitis is an inflammation of the internal tissues of the tooth (pulp), containing nerve, blood vessels and connective tissue cells.
- Periodontitis is the process of spread of harmful microorganisms into the canal and the tissues surrounding it.
These diseases are usually accompanied by certain symptoms:
- Severe persistent pain in the tooth , characteristic pulsation, intensifying in the evening and when biting on the tooth.
- Swelling and discoloration of the gums , the formation of an abscess or fistula on it.
- Halitosis.
It is also possible that there will be no significant symptoms due to the death of the pulp. Only immediately after an examination in the chair, a specialist can accurately determine whether endodontic treatment of dental canals will solve the problem that has arisen and select the most effective therapeutic regimen. Our clinic strives to provide services at the highest level, so at Implantmaster it is possible to treat tooth canals under a Labomed Magna microscope. The success rate of treatment of complex canals increases significantly.
Other indicators for the removal of baby teeth
- Caries, which can develop on the teeth of a two-year-old child. The resulting carious cavity can become a source for the spread of infection.
- Inflammation of the pulp, which occurs against the background of advanced caries.
- Periodonitis. Inflammation of the soft tissues around the tooth.
- This disease occurs in 3-5% of children.
- Trauma, as a result of which the tooth became loose and part of the tooth broke off. When a tooth is injured, the nerve bundle often ruptures. The pulp becomes unviable and must be removed.
Methods of treatment of dental canals
In dental practice, there are two main methods of treating tooth root canals:
Therapeutic (biological), in which the entire pulp or part is preserved. A drug with a medicinal effect is placed into the dental cavity, which separates the pulp from the temporarily installed filling material. Also, medications can penetrate through dentin from dressings with an antibacterial drug. The effectiveness of drug therapy appears only at the very beginning of inflammation.
Surgical (pulp extirpation) - removal of all pulp from the canals, cleaning, processing and dense filling of the canals. The canals are treated using one of the possible methods:
- Standard filling is the introduction of a paste-like material into the root canal cavity;
- Vertical condensation method - by compacting gutta-percha in a filling paste;
- Filling with thermophile - hot gutta-percha is placed on the obturator and fills all branches.
Sometimes, for endodontic intervention, it is advisable to perform resection of the root apex - if a granuloma, fibroma, cyst, or other complications are detected around the root apex.
How painful is root canal treatment?
Unpleasant sensations in the tooth occur under the influence of microorganisms on the vessels and nerve at the root. Cleaning the canals and removing the inflamed pulp eliminates pain. With the use of modern anesthetics, endodontic treatment proceeds comfortably. Treatment of 1 tooth canal lasts about forty minutes (depending on the complexity of the root anatomy); a three-canal tooth may require about two hours. In our clinic, doctors carry out all procedures for root canal treatment at a reasonable price using a rubber dam to limit the working field and ensure comfort for the patient.
Are there nerves in baby teeth?
The structure of baby teeth is similar to the structure of permanent teeth:
- The outside of the tooth is covered with one of the hardest tissues of the body - enamel. The tooth is additionally covered with a cuticle - a membrane that wears off when chewing food;
- There is bone tissue under the tooth. It is the basis of the tooth and is located around the root of the tooth;
- the canal and crown are filled with pulp, in which numerous capillaries and nerve endings are intertwined. Milk and molar teeth begin to form in the child, who is still in the womb of the mother. Medical research has proven that these teeth already have roots and nerves.
By the time a child’s first teeth begin to erupt, their roots have already dissolved. Milk teeth are destroyed under the influence of acids found in food, pathogenic microorganisms and mechanical damage. A child's first teeth are covered with a thinner layer of enamel, so they hurt, just like adults.
If your tooth starts to hurt, don’t delay your visit to the pediatric dentist. Inflammation may begin, which will affect the gum tissue, and tooth treatment will be more painful.
Stages of dental root canal treatment
Tooth canal treatment is performed using different methods. Initially, a diagnosis is made and a treatment plan is drawn up. Root canal treatment is a very painful process, so anesthesia is required, agreed upon with the patient. An anesthetic injection is given into the gum of the disturbing tooth. After isolating the working field with a rubber dam, the doctor begins the main stages of root canal treatment:
1 . Extraction of affected dentin . An approach to the root canals is provided by opening the dental cavity and sawing off the overhanging edges to gain access to the mouths of the canals. In case of pulpitis of a tooth with several roots, persistent pain may be experienced, then the first visit to the doctor ends with the opening of the tooth cavity and the introduction of devitalizing paste. A temporary filling is placed on top.
2 . Removal of coronal pulp . The second visit is already painless, because... the devitalizing paste will work. With periodontitis, at the time the dental cavity opens, the canals may already be opened or the destroyed pulp may need to be removed. This stage is called devital amputation. In case of pulpitis, under the influence of an anesthetic, partial extraction of the “living” pulp is carried out - the stage of vital amputation.
3 . Channel processing . The canals are cleaned and expanded to remove microorganisms and prevent them from entering the dentin. Wash the putrid masses using solutions with hydrochloride for disinfection. Next, the canals are dried and filled with a medicinal preparation.
4 . Filling the canals is the last step of effective treatment.
When treating root canals of teeth, the price includes each material separately. Therefore, the cost of root canal treatment depends on the chosen filling component.
How channels are processed
The effectiveness and duration of endodontic treatment depends on the method of canal treatment chosen by the doctor, namely:
- Manual - cleaning using special tools; the process is lengthy and tedious not only for the patient, but also for the doctor.
- Mechanical - cleaning using nickel-titanium tools and an endomotor; Much faster and more efficient than manual cleaning, it allows you to clean even curved channels well.
- Ultrasonic – cleaning using an ultrasonic scaler; special endodontic attachments make it possible to easily remove remaining pulp and quickly expand narrow canals; with the help of such attachments, it will not be difficult to free the canal from old gutta-percha or remove a broken instrument.
Most experts agree that high-quality irrigation of dental canals can only be achieved by combining different methods.
Important!
In our clinic, the endodontist has the opportunity to use mechanical and passive ultrasonic cleaning in his practice, which, in combination with competent medicinal treatment of the canal with special disinfectants, ensures a 100% result.
The main principle of qualified endodontic treatment is the use of a microscope, which allows, under multiple magnification, to achieve the necessary efficiency of treatment, thorough disinfection and sealing of canals.
To control the quality of the work done during treatment and after its completion, control images must be taken to exclude the possibility of complications.
Treatment of tooth canals under a microscope
One of the most advanced methods in endodontics is root canal treatment under a dental microscope. Powerful optics increases the view many times over; given the channel diameter is no more than 1 mm, it is very difficult to process it efficiently without magnification.
Advantages of dental treatment under a microscope:
The doctor clearly sees the structural features of the canal mouths, every deviation from the direction, which is important when the root canal has a non-standard shape. The microscope makes it possible to preserve healthy tissue by removing only diseased tissue. Thanks to the targeted examination of tissue under the Labomed Magna dental microscope, which is available in the clinic, our highly qualified specialists will ensure the best outcome of the intervention, eliminating the likelihood of problems and complications.
Using a dental microscope allows the dentist to successfully solve any complex clinical problem. At the Implantmaster dental clinic, tooth canal treatment under a microscope is performed at affordable prices, which can be found on the website.
Read more about dental treatment under a microscope »
Recommendations after root canal treatment
Root canal treatment with mechanical instruments demonstrates high success rates. After the manipulations, you must follow the recommendations:
- Due to the preservation of the reaction to irritants, it is worth excluding the consumption of hot, cold and spicy foods for a while.
- Maintain good oral hygiene - in addition to brushing your teeth in the morning and evening, use dental floss and irrigator.
- Do not eat solid foods (nuts, candies, etc.), because The tooth may be destroyed or the root canals may be damaged.
- Have a medical examination at the dentist (once every six months).
After the procedure, tooth sensitivity increases due to the tissue reaction to the filling material. The discomfort will disappear after a few days.
The nuances of filling temporary teeth
Temporary teeth are prepared in much the same way as permanent teeth. When a cavity is created during cleansing of a carious lesion, it is acceptable to leave hard, dry dentin, even if it is slightly pigmented. Since this indicates low activity of the carious process. Otherwise, there is a possibility of accidental penetration into the pulp. Given the characteristics of dentin such as moisture and friability, it is necessary to completely clean the cavity.
Temporary units are filled using atraumatic chemical-mechanical methods to prepare the cavity for restoration. This affects children's ability to adequately accept dental treatment and not be afraid of going to the doctor, as was the case many years ago. The sound of the drill does not terrify the child, does not make him afraid in anticipation of painful sensations.
The use of a drill is justified in cases of large tissue damage, when it is impossible to achieve complete treatment of the cavity from a carious defect by mechanical or chemical means. An important factor in the treatment of caries is sedation. If it is possible not to use it, the doctor will not do so. But if it is necessary to numb a tooth, the dentist must, together with the anesthesiologist, select the correct dose of anesthetic.
If the treatment area is several units, a decision is made on general anesthesia or sedation, when the child is conscious, but does not experience pain and can perform the actions that the doctor tells him during the treatment process.
Children under 2 years old cannot sit in the dentist's chair for a long time, so the doctor needs to act quickly, competently, and painlessly. The child needs a pediatric dentist. An adult will not be suitable, since in pediatric dentistry special instruments and preparations are used, doctors take into account the anatomical features of the structure of the organ, as well as psychological aspects to relax the child at the doctor’s appointment.
What materials are used (which fillings are best placed on baby teeth)
Filling materials for baby teeth,
suitable especially for children, used if conservative treatment does not help. It may also be that it is ineffective at this stage of the disease. It is important for parents to understand what fillings are used, whether there is a difference between them, the cost of the material, its effectiveness, and what reviews the formulations used have received.
On the dental portal you can see children's dental clinics, reviews of doctors, and videos about filling mammary units. To understand the compositions currently used in pediatric dentistry, let’s look at them.
Composite photopolymers
This material hardens in the cavity under the influence of a light lamp. They aesthetically match the color of the patient’s enamel, protect against the spread of caries, and are an expensive technique. Installed in the smile area to achieve the cosmetic effect of invisibility of the filling. Widely used on anterior units to achieve a cosmetic defect. Produced on the basis of silicon dioxide. They have some toxic effects on pulp tissue, so they are used with caution for pulpitis.
In terms of service life - they have great strength, they last until the change of the milk permanent bite. The disadvantage of their use is the need for anesthesia. Not used if the patient does not maintain hygiene, does not brush his teeth well, and there is acute caries in the cavity. The disadvantages of use are also the weak shrinkage.
It is established when the patient can sit quietly in a chair and allows the doctor to carry out manipulations to thoroughly clean the cavity from caries. For this reason, children under 2 years of age are not suitable patients for installation of this type of filling.
Glass ionomer cement
It consists of powdered glass and polyacrylic acid, which hardens when the components react acidically with each other. Glass ionomer cement for filling baby teeth
widely used on the chewing surface. The composition includes fluoride ions that work to remineralize the enamel. This type of material does not have strong strength, but it will last for several years until the bite changes. A child does not have such a strong chewing load as an adult, so the use of glass ionomer cement is justified. They differ in composition in some components, in their area of application - for strengthening fabrics and for aesthetics.
It has good adhesion to the tissues of the organ itself and other materials used for filling, protection, and strengthening of walls. Protects against the spread of caries and bacteria. Reviews from dentists who use glass ionomer material confirm the good properties of this cement: it does not stain when it comes into contact with coloring products, and its strength is sufficient for the entire time until the bite changes.
Colored compomers
Colored compomers are a great way to correct a tooth defect and involve your child in the process. The cooperation of a young patient with a dentist leads to positive results: the child is not afraid to have his teeth treated and visit the doctor, the doctor does his job efficiently, without making the child nervous. A colored filling gives the child the opportunity to take his mind off the unpleasant process, participate in choosing the color, make his own decision, feel responsible and allow the doctor to finish the job.
Colored fillings require chemical preparation of the cavity before installation. The doctor does everything quickly: cleans the cavity, etches it with 35% orthophosphoric acid for a minute, applies a compomer, then polymerizes and polishes it. The whole process takes about 15-20 minutes. During this time, the child will not get tired, and will be motivated to come to the appointment next time and choose a different color of filling if the need for treatment arises.
Colored compomers are placed on the chewing surface. The material is characterized by high plasticity, fills the entire space in the cavity, has the property of releasing fluoride to the enamel, as well as accumulating it from products. The low price allows you to economically treat caries in a child. Today the material is presented in the following colors: blue, gold, yellow, green, silver, orange, pink.
Preventive measures
The well-known phrase that preventing a disease is cheaper, better, more convenient than treating it afterwards also applies to teeth. Preventative measures are ways to care for the oral cavity and take care of the health of the milk units. This will ensure a healthy permanent bite. Taking care of your baby's dental health begins with the mother's health during pregnancy.
- While breastfeeding, you need to maintain your health and take minerals to strengthen your enamel.
- Child’s oral hygiene after feeding, use of cleansing wipes and fingertips for the smallest children, special toothbrushes and pastes.
- It is important for adults to remember: you should not lick a child’s spoon, caries develops due to the presence of bacteria, and they are transmitted from adult to child.
- A balanced diet, the presence of dairy products and fish, a minimum content of carbohydrates and sweets.
- Accustom your child to self-hygiene, ensure that he does it efficiently and regularly, and achieve automaticity of a useful habit. In the morning and evening - brush your teeth, rinse your mouth - in the afternoon after meals.
Regular preventative visits to the dentist will help avoid a big problem. In the early stages, caries responds well to mechanical impact on the enamel, which does not leave a mark on the enamel tissue and stops the pathological process. The tissue does not need to be prepared. Preservation technique in the early stages will allow baby teeth to remain in the jaw all the time until they are due to be replaced by permanent ones.
Tooth hurts after root canal treatment
If after root canal treatment the tooth hurts when pressed, then this may be normal. Unpleasant feelings are associated with a small amount of pain relief in the area of the causative tooth. The next probable reason is the excessive impact of the instrument when cleaning the canal, with its likely insertion beyond the apex of the root.
From time to time, unpleasant sensations occur for several days from the very impact on a small area or when a lot of filling material is introduced into the canal, pressing on the walls. As a result, the tooth may “sink” even after treatment. But pain after canal filling indicates that it is advisable to repeat the visit to the doctor.
Possible complications after root canal treatment
Sometimes treatment does not go smoothly and complications arise:
- Perforation is the appearance of cracks in the walls of the canals. The solution is treatment with medications and filling.
- Cheek swelling. The reason for the swelling of the cheek after root canal treatment is the penetration of the anesthetic into the periodontal tissues and mucous membranes, which easily absorb liquid.
- Tool failure. The files that process the canal walls are thin jagged needles. If it breaks during the necessary actions, the fragments are removed by specialized devices. Innovative tools are made from nickel and titanium alloys; they are more wear-resistant and durable.
- Adverse reactions to medications. The spectrum and their effects on topical anesthetics are minimized. Before administering drugs, the doctor must collect data on drug intolerance - so the possibility of allergies is close to zero. Moderate and minor adverse reactions are most often short-lived and can be overcome by replacing the drug.
- Other complications. Accidental swallowing of pieces of filling material, dust from teeth, and small instruments is now essentially non-existent due to the use of a rubber dam - a latex scarf that isolates one to several teeth from the oral cavity.
In what cases is a tooth removed after root canal treatment?
In some circumstances, it is necessary to part with an endodontically treated tooth. Often a disastrous result is justified by the following factors:
- Unsatisfactory quality of root canal treatment with further intractable infection;
- Examples of treatment of “eights”, due to the atypical anatomy of the canals;
- Complicated structure of the patient’s canals;
- Failure of a patient to visit a dentist in a timely manner to provide specialized care, when the necessary medical procedures do not lead to an effective outcome.
Prices for root canal treatment
Treatment of caries by filling tooth surfaces
- Anesthesia
- Cavity preparation (preparation, medicinal treatment, application of a gasket)
- Filling with light-curing composite
- Grinding and polishing the filling
- X-ray images
Price : from 3,000 ₽ to 8,050 ₽, depends on the number of tooth surfaces affected.
Treatment of caries by placing a ceramic inlay “E-MAX” or “CEREC” or “EMPPRESS”
| from 20,000 to 28,000 ₽ |
Unsealing all tooth canals
| from 4,000 to 8,500 ₽ |
Filling all tooth canals
| from 6,500 to 11,500 ₽ |
| Removing a foreign body from a tooth canal (pins, fragments of instruments, etc.) | 3 000 ₽ |
| Application of medicinal paste into the tooth canals | 2 000 ₽ |
| Sealing tooth fissures | 2 000 ₽ |
| Treatment of caries without drilling the tooth using the “Icon” method | 3 000 ₽ |
| Complete restoration of a tooth with a light-curing composite (Tooth restoration) | 9 500 ₽ |
The cost depends on many factors: the degree of destruction of hard tissues, the number of roots and canals in them, and treatment methods. The prices for the service provided are relatively high due to the structural features of the roots of the teeth - they are narrow, thin, branched, requiring the doctor to have high precision and professionalism. The cost of manipulations, which include root canal treatment, is announced to the patient at the first visit; for the most part, it is free. To clarify the diagnosis, an X-ray is taken, and at the end of treatment a final image is taken.
The cost of treatment for a single-canal tooth starts from 15,000 rubles. One visit involves using a microscope for 30 minutes and not using medicinal paste. If the tooth has previously been treated, then a filling is added, the cost of which varies from 1,500 rubles to 2,500 rubles for 1 channel. Therefore, endotherapy of a tooth starts from 16,500 rubles for a single-canal tooth in one visit. The price for dental treatment with 2 or more canals increases significantly. In such situations, the doctor pays separate attention to each canal, spending more of his time and filling composite.
Root canal instrumentation techniques in different age groups: a comprehensive narrative review
Introduction
As the world population grows, there is both an increase in life expectancy and a decrease in tooth loss. Because root canal treatment is performed on patients of all ages, clinicians should be aware of differences in root canal system morphology and dentin structure depending on patient age.
It is known that it is almost impossible to create guidelines or instrument calibers that would guarantee adequate root canal preparation in any age group. However, due to differences in canal morphology and dentin structure, as well as the use of different endodontic instruments and techniques available today, the clinician may use different methods to instrument the root canal system. Meanwhile, various tools—especially canal shaping files made from different heat-treated alloys with different geometric characteristics—are reported to have distinctive mechanical properties and resulting positive processing results. The choice of instruments may lead to inadequate clinical results in certain cases, depending on the properties of the instrument and the clinical condition of the patient, including age. Therefore, the purpose of this article is to review age-specific clinical guidelines for root canal instrumentation techniques through a literature search and review.
Review and search of literature
An electronic literature search was conducted, including MEDLINE (Ovid), PubMed, and Web of Science databases. The search used dictionary terms and arbitrary phrases, such as: “root canal treatment depending on age”, “root canal instrumentation depending on age”, “chemomechanical preparation depending on age”, “clinical recommendations in endodontics depending by age”, “toolkit for root canal treatment at different ages”, “geriatric root canal treatment” and “childhood root canal treatment”. However, a review of the literature revealed a lack of studies with practical clinical recommendations when selecting appropriate instruments for age-related root canal treatment.
Therefore, a comprehensive review of canal morphology, dentin structural characteristics, and endodontic outcomes in different age groups was taken from articles that were published from 1925 to 2018, rather than a systematic review. Previous studies have used different approaches to classify age-related morphological and structural changes, either based on statistics (to ensure a larger sample size) or without explanation of the classification. This review categorizes age differences into the following age groups: persons aged 20 years or younger, 21 to 40 years, and 41 years or older.
Morphology of root canals depending on age
- Contour and cross-sectional diameter of the channel
Differentiation of the root canal system due to the deposition of secondary dentin is an age-related process. With age, the pulp cavity usually decreases in size (Fig. 1).
Rice. 1. Panoramic radiographs showing the size of the pulp chamber and root canal depending on age. (A) Persons under 20 years of age (13 years), (B) persons between 20 and 40 years of age (39 years), (C) persons over 40 years of age (64 years). Image (A) shows the large pulp chamber and the direct direction to the canal opening. Image (B) shows the denticulate area and the direction at an angle to the canal orifice. Image (C) shows a small area of the pulp chamber and sclerotic canals.
Typically, people under the age of 20 have roots with one large root canal (mostly oval). Median mesial canals in mandibular molars are found mainly in individuals under 21 years of age. Individuals between the ages of 20 and 40 have several separate canals in one root. The number of root canals was found to increase mainly in the maxillary and mandibular second premolars, the distal root of the mandibular first molars, and the mandibular incisors. In patients over 35 years of age, more round canals were found in the mandibular second molar, while in those under 35 years of age, more oval canals were found.
The C-shaped configuration (type III) is more common in mandibular molars in individuals under the age of 40. In a study using cone beam computed tomography, patients younger than 42 years were 4 times more likely to encounter a mesial canal than patients older than 42 years. In people over 40 years of age, the deposition of secondary dentin leads to a decrease in the diameter of the canal and the disappearance of additional canals. Fewer canals were found in individuals aged 51–70 years. For example, in this age group, the absence of the second mesiobuccal canal in the maxillary molars was observed.
- Isthmuses
The incidence of canal isthmuses appears to be related to age. People under 20 years of age have wide and oval canals without isthmuses in the early stages of root development. In people aged 20 to 40 years, the deposition of secondary dentin in the mesiodistal direction leads to the formation of 2 canals with an isthmus. Up to 81% of mesial roots of mandibular first molars in individuals aged 20-39 years have isthmuses, especially at a distance of 4-6 mm from the apex. In persons over 40 years of age, the extent and number of isthmuses are significantly reduced, and the canal is completely separated. In people over 50 years of age, the incidence of isthmuses was 16.7%, and only 24% of people over 60 years of age had isthmuses in the mesial roots of mandibular molars. The ratio of partial isthmuses to complete isthmuses increases with age. Figure 2 shows isthmus characteristics in different age groups with cone beam computed tomography images.
Rice. 2. Cone beam computed tomography: three images of the mandibular first molar showing isthmus characteristics in different age groups. (A) Persons under 20 years of age (18 years): wide canal without isthmus, (B) persons 20 to 40 years of age (38 years): isthmus in the mesial root, (C) persons 40 years of age or older (62 years) : sclerotic mesial canals without isthmus, similar to one canal.
Age-related changes in dentin structure
With age, normal dentin undergoes physiological changes and turns into transparent (sclerosed) dentin. As the tooth matures, peritubular dentin becomes more mineralized and a decrease in the average number of dentinal tubules is observed. The process of mineralization and dentin sclerosis lead to narrowing of the tubules. In some cases, this process can lead to complete obliteration of the dentinal tubules. Mineralization begins in the third decade of life in the apical zone and develops coronally with age.
The penetration of bacteria into dentinal tubules may be a determining factor in their virulence in the root canal environment. Microbial diversity and microbial load are higher in young people and decrease with age. This decrease may be due to mineralization of the tubules, as well as a decrease in the space of the pulp cavity, isthmuses and accessory canals. Dentinal tubules typically have a larger diameter than the average diameter of Enterococcus faecalis (E. faecalis) cells by approximately 0.8–1 nm. However, due to age-related mineralization of the tubules in old age, the depth of penetration of E. faecalis into dentin through sclerotic or obliterated tubules decreases. On average, bacteria penetrate 65 microns less deeply in people aged 60–77 years than in people aged 18–24 years.
With age, the water content of dentin decreases and collagen modifications, such as cross-linking, increase. Because of these age-related changes, resistance to dental damage decreases in older adults, but significant reductions in dentin strength and fracture strength result in an increased incidence of vertical root fracture (VRF). VRFs are most common in posterior teeth in patients between 40 and 60 years of age. In addition, the growth rate of vertical cracks in “old” dehydrated dentin is 100 times higher than in “young” hydrated dentin. Pre-existing dentinal microcracks in endodontically untreated roots become more common with age (8.3% in persons over 40 years of age, 3.7% in persons over 20–39 years of age). In contrast, in individuals under 20 years of age, the dentin walls are thin, which can lead to coronal or root fractures of the tooth under normal functional stress.
Results depending on age
Data on the effect of patient age on the results of endodontic treatment are contradictory. Some studies reported that age had no statistically significant effect on results, while others stated that patient age significantly affected results. Some studies have shown that treatment in older patients had a higher success rate than in younger patients, while other researchers have found better results in younger patients and have demonstrated that age is a risk factor for complications. For example, older patients are 1.4 times more likely to have teeth removed after root canal treatment. The rate of subsequent removal increases by 1–2% each decade until it reaches a plateau after age 60.
These better results in older people can be explained by the gradual reduction of the pulp space, the disappearance of additional canals and isthmuses and the narrowing of the dentinal tubules up to complete obliteration. These changes limit the volume available for infection, which ensures adequate cleaning of the canal, as well as its formation and medicinal treatment. Reports of better results in younger adults may be explained by the increased prevalence of apical periodontitis with age, which is associated with a lower likelihood of successful endodontic treatment. Another explanation could be that older people have slower and less efficient healing processes or longer healing times. Immunological changes that occur due to aging include changes in pulp cells expressing macrophage-associated antigens. Aging is associated with low levels of expression of genes encoding transcription regulators and high levels of expression of genes involved in apoptolytic processes.
In addition, systemic diseases are more common in older age groups, and it has been reported that some systemic diseases may be associated with endodontic treatment outcome. Diabetes (non-insulin-dependent or insulin-dependent) or an impaired nonspecific immune response leads to decreased success of endodontic treatment in patients with preoperative periradicular lesions.
Table 1 shows the characteristics of canal morphology and dentin structure in different age groups, including the contour and cross-sectional diameter of the canal, the presence and characteristics of isthmuses, accessory canals, the number and diameter of dentinal tubules, and sclerotic dentin. Taken together, these age-related changes suggest that clinicians may choose different clinical approaches for different age groups.
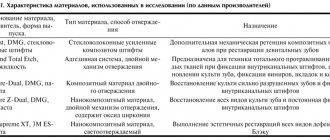
Table 1. Characteristics of the canal morphology and dentin structure in different age groups.
Possible clinical suggestions
Within the limitations of the studies that were reviewed, the following possible clinical recommendations for root canal instrumentation can be made. For persons over 20 years of age, the recommendations are as follows. Large channels do not require additional expansion. Scraping instruments may be preferred to clear the root canal wall of biofilm while simultaneously activating the irrigation solution. Possible tools: Self-Adapting File (SAF; ReDent, Ra'anana, Israel) and XP-Endo Finisher (FKG Dentaire, La Chaux-de-Fonds, Switzerland). These systems are effective in cleaning a relatively large and oval canal lumen with a cleaning action while constantly changing the irrigant for SAF or eccentric movements of memory-controlled instruments such as the XP-Endo Finisher.
For persons aged 20 to 40 years, the following recommendations exist. The channels are generally open and difficulties in creating a carpet are rare. In these root canal systems, conventional nickel titanium (NiTi) rotary systems can be used to shape the canal to size #30–#35 followed by sodium hypochlorite activation. Possible instruments: ProTaper Next (Dentsply Sirona, Ballaigues, Switzerland), XP-Shaper (FKG Dentaire, La Chaux-de-Fonds, Switzerland) and 2Shape (MicroMega, Besançon, France). The use of scraping instruments in this age group may be considered in oval canals.
For people who are 40 years of age or older, the recommendations are as follows. In these root canal systems, after using stainless steel hand K-files (#06, #08 and #10), the NiTi system can be used to create a carpet. Possible tools include G-File (MicroMega), PathFile (Dentsply Sirona), OneG (MicroMega), ProGlider (Dentsply Sirona), Scout RaCe and Race ISO 10 (FKG Dentaire). Thereafter, expansion of the apical diameter of the root canal to size No. 30 or No. 35 is preferably carried out using NiTi instruments, which place less stress on the dentin. Possible instruments for this purpose are instruments with a smaller cross-sectional area (MTwo [VDW, Munich, Germany], Race [FKG Dentaire], ProFile, 2Shape), instruments with a smaller taper (0.02 and 0.04) (Race, ProFile ) ) and made from flexible NiTi (memory controlled file), such as HyFlex (Coltene/Whaledent, Inc, Cuyahoga Falls, OH, USA) and Typhoon (Clinician's Choice Dental Products, New Milford, CT, USA).
Table 2 presents the proposed algorithm for root canal instrumentation in different age groups. The current suggestions are based on available evidence and reflect the limitations of the studies that were included in the review. However, no single algorithm fits all teeth. The clinician may encounter inconsistencies between chronological age and biological age. Pathological or iatrogenic factors can change the contour and cross-sectional diameter of the canal. These factors include carious lesions or extensive restorations, attrition or attrition, occlusal trauma, periodontal disease and treatment, and orthodontic treatment. The irritants that each tooth encounters during its life must be taken into account due to the possible rapid increase in reaction and dentin deposition. In contrast, pulp necrosis in younger patients due to trauma or caries can lead to the formation of wider canals with thin dentin walls as these patients get older.
Table 2. Algorithm for root canal instrumentation in different age groups.
The contents of this review do not necessarily support any specific technique for specific clinical situations in patients of various age groups and root canal conditions. However, it may be generally acceptable to emphasize the importance of chemomechanical preparation, which always improves canal clearance through shaping and activated irrigation, regardless of the patient's age and canal condition. Correct assessment of root canal morphology, coupled with an adequate understanding of the influence of age on these characteristics, can help the clinician select the most appropriate instrumentation technique and irrigation activation.
conclusions
The current review examines age-related differences in canal morphology, dentin structural characteristics, and endodontic outcomes. Depending on age, clinical recommendations for instrumentation should ideally be based on a systematic review of randomized controlled trials, taking into account the quality of evidence and patients' values, preferences and financial resources. However, no studies suitable for this purpose have been conducted. Thus, the present article is the first attempt to interpret age-related morphological and structural changes and make practical clinical suggestions within the limitations of existing studies.
A systematic review is a comprehensive method of finding relevant studies on a specific topic, and then the identified studies are assessed and summarized according to a predetermined and explicit method. In contrast, narrative review is a traditional method of peer review. This method is subjective and there are no formal rules for selecting studies or standard statistical methods for pooling studies. Therefore, when reading and evaluating a narrative review, readers should keep in mind that the author's bias may or may not be present.
An additional limitation of these proposed clinical offerings is that the aforementioned tools are not available to all clinicians due to local market conditions and financial resources. Future research should examine the influence of patient age on other aspects of root canal treatment (eg, access cavity preparation, irrigation techniques, and obturation techniques). It can be concluded that the clinician's awareness of age-related differences in root canal morphology and dentin characteristics may influence the choice of instruments for root canal treatment.
Source : Restorative Dentistry & Endodontics
Translation by Tatiana Chuiko for the BELODENT.ORG portal
Cost of root canal treatment under a microscope
The patient should be prepared that root canal treatment using a microscope in Moscow will be more expensive than classical treatment. This service is not available in all clinics. The endodontist uses expensive equipment to increase access to the canal several times. The doctor first undergoes specialized training. All this affects the final price for root canal treatment in Moscow under magnification - from 7,000 rubles to 20,000 rubles. A repeated request for dental canal treatment using a microscope increases the cost of the service by an average of 3,000 - 5,000 rubles, depending on the number of canals.
Author:
Stages of endodontic treatment
- Diagnostics. If there is a suspicion of problems in the dental canal, an x-ray is taken. The specialist can also study the images that the patient already has. Depending on the diagnostic indications, treatment is selected.
- Pulp removal. First, the dentist anesthetizes the tooth. Then he opens it and removes all damaged tissue. Next, the cavity is given a convenient shape. Then the channels are disinfected using a special solution.
- Root canal filling. The cavities are filled with special materials. They are divided into hard (pins), hardening (various cements) and plastic (paste or gutta-percha). The most modern are the latter.
- Tooth restoration. This is the restoration of the shape of a tooth using a filling, crown or inlay.